Head and neck
Vol. 46: Issue 3 - June 2026
Modular approach to the parapharyngeal space based on transoral robotic surgery
Authors
giacomo pietrobon
 , Stefano Filippo Zorzi
, Francesco Bandi
, Francesco Chu
, Chiara Mossinelli
, Francesca Ruju
, Gioacchino Giugliano
, Mohssen Ansarin
, Stefano Filippo Zorzi
, Francesco Bandi
, Francesco Chu
, Chiara Mossinelli
, Francesca Ruju
, Gioacchino Giugliano
, Mohssen Ansarin
Summary
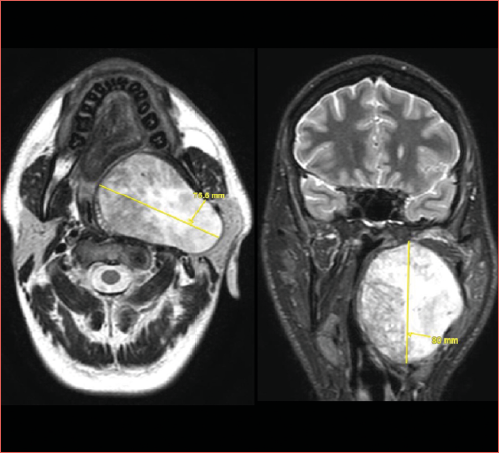
Cover Image
Objective. Lesions of the parapharyngeal space can be resected through a variety of approaches, depending on their location and biology, as well as on the surgeon’s experience. Historically, the transcervical approach has been the most employed, while the transoral has been neglected because of its intrinsic limitations. The advent of robotic surgery has expanded the indications of transoral resection thanks to its reduced morbidity and the possibility of combination with other accesses.
Methods. We conducted a retrospective analysis of patients submitted to transoral robotic surgery (TORS) for parapharyngeal lesions at the European Institute of Oncology. We further focused on patients treated with a combined transoral-transcervical approach.
Results. Between 2013 and 2024, 43 patients underwent TORS for a parapharyngeal lesion, with curative intent in the majority of cases (93%). In 9 cases (19%), a transcervical/transparotid approach was combined with TORS. A transmandibular approach was never necessary. The postoperative course was uneventful for all patients. The majority of lesions were benign (79%).
Conclusions. TORS has proven to be a viable option for lesions of the parapharyngeal space. A combined modular approach is feasible to lessen surgical morbidity.
Introduction
The parapharyngael space (PPS) is a pyramid-shaped deep-located suprahyoid infracranial fascial plane with a close relationship with adjacent spaces and organs (masticator space, parotid space, pharynx). Historically divided into pre-styloid and post-styloid, nowadays, authors refer to true parapharyngeal space (previously pre-styloid) and carotid space (previously post-styloid). Moreover, the PPS may be further subdivided into three sub-compartments (superior, middle and inferior), as proposed by Prasad et al. 1.
Tumours arising in this region are rare and mainly benign, derived from salivary glands or neural structures 2,3. Accordingly, benign lesions may grow extensively in the surrounding soft spaces, causing dislocation of neighbouring structures and even clinically-evident swelling, but they typically do not infiltrate or present a clear cleavage plane. For all these reasons, surgery is the mainstay of the treatment of these lesions, and it should be thorough and as conservative as possible.
Several different surgical approaches have been proposed throughout the years, with the transcervical one being the most adopted2. Ferrari et al. recently published an extensive anatomic study, which enlisted all the existing approaches (classified in “anterior” and “lateral”) and quantified the exposure rate of each PPS subunit through coloured radar plots 4. The same authors later proposed a surgical algorithm to choose the most suitable approach to PPS, based on their retrospective analysis of 153 consecutive cases 5. The transoral route was used in only 1.3% cases, which is explained by the limited exposure granted, also highlighted in the radar plot. Similar data (2%) were shown earlier by Riffat et al. in their systematic review on publications up to 2009 2.
The introduction of robotic surgery in 2009 has revolutionised and boosted the transoral approach to PPS, as demonstrated by increased numbers in systematic reviews from 2014 to 2021 6,7, in a high-volume single-centre cohort 8 and also in our personal experience 9. In the era of minimally-invasive approaches, the transoral robotic surgery (TORS) not only reduces surgical morbidities, but also may be part of a combined increasingly-morbid approach 10, providing both surgeons and patients with the possibility of demoting, but also not precluding more aggressive procedures to a last-resort situation. In particular, TORS may be combined with a transcervical approach in cases where the lesion extends superiorly (less than 1 cm to the skull base) and laterally (beyond the stylomandibular ligament), as suggested by Boyce et al. 11. The transoral and transcervical access can be complementary to surgically dominate the lesion, with each route overcoming the limitations of the other. Moreover, and more importantly, a transmandibular approach may be avoided, even in cases of massive benign primary tumours (Cover figure).
In this paper, we aim to present our experience in parapharyngeal lesions treated with TORS combined with a transcervical/transparotid approach, and to speculate on the advantages and shortcomings of the procedure, as well as its indications and contraindications.
Materials and methods
We retrospectively reviewed the database of TORS from July 2007 to November 2024 at the European Institute of Oncology and selected patients treated for a PPS lesion. Out of this initial cohort, we further selected patients treated by TORS combined with a transcervical or transparotid approach. Data on patient demographics, hospitalisation, tumour extension and histology, success of the surgical procedure, and rate of perioperative complications were collected. We also retrieved data on previous surgical approaches, if available, and the steps of our surgical procedure.
Results
Between 2013 and 2024, 43 patients underwent TORS for a parapharyngeal lesion, which was benign in the majority of cases (34, 79%), with pleomorphic adenoma representing about half of the cohort (23, 53%). In 40 cases (93%), the surgery aimed to completely remove the lesion and it was successful in 38 cases (31 benign, 7 malignant), while in 2 patients (5%) a macroscopic residue of a benign tumour was left because of the impossibility of further resection due to adhesion to the skull base (myoepithelioma) or the parotid gland (pleomorphic adenoma), which had not been anticipated by preoperative imaging. In particular, tight adhesion of the myoepithelioma to the skull base was not evident preoperatively, despite attentive imaging and a multidisciplinary revision of such a challenging case, which is the current practice in our institution and should be mandatory in all complex surgeries, independently of the technology available.
In both cases, given the nature of the lesion and the morbidity of a transmandibular or transparotid access, a minimal residue was deemed acceptable. To note, in the remaining 3 cases (7%, 2 malignant and one benign), surgery aimed to simply sample the lesion (Tab. I).
In 9 cases (19%), a transcervical (n = 8) or transparotid (n = 1) approach was combined with TORS, either ahead of it (n = 3) or after (n = 6). Due to the size and shape of the masses, all these 9 cases would have undergone a trans-mandibular approach, if TORS had not been available. All the combined procedures were completed successfully and a mandibulotomy was never necessary.
In 5 cases (6%) of the overall TORS cohort, the adenoma was removed in fragments, while in 5 additional cases a capsule damage occurred. Four of these events (3 capsule damage, one fragmentation) occurred in the combined procedure (lesion major axis: 37, 50, 55, 80 mm).
In the subcohort (TORS combined), all patients underwent tracheotomy to secure the airway in the postoperative period. These cases would have potentially required a transmandibular approach, and thus the same airway protection. The tracheal tube was removed after 5 to 7 days. Of note, in the exclusive transoral approach, a tracheotomy was performed in 25 cases (74%). This significant number is explained by the excessive prudence in the early years of our experience. The decision was primarily based on the risk of postoperative oedema (pharynx and tongue) and bleeding.
In 6 cases, a nasogastric tube (NGT) was placed that remained for 5 to 6 days. No gastrostomy was required. In all cases, a cervical drainage was placed to ensure negative pressure, and was kept in place for 3 days. The post-operative course was uneventful for all patients, who were discharged after 7 to 9 days. Postoperatively, one patient presented Claude-Bernard-Horner syndrome and mild transient impairment of the marginal mandibular branch of the facial nerve; another had cervical wound haematoma; lastly, one had an oral incision dehiscence. This last case was managed conservatively: fibrin glue was injected into the small residual cavity, and oral reuptake was maintained with the usual schedule.
To note, the suture of the pharynx is realised with a multilayer technique, so that the tension on the mucosal layer is decreased. In case the void is excessive, a buccal fat pad flap may be rotated posteriorly to fill in the gap. This flap was never necessary in our cohort.
All lesions were benign (7 pleomorphic adenomas, one myoepithelioma), except for one (carcinoma ex pleomorphic adenoma). At last follow-up (range 2-84 months, 58 months for carcinoma), 8 patients were free of disease; one patient (myoepithelioma) had persistent but stable disease, which was further treated with radiotherapy because of an initial regrowth, revealed by magnetic resonance imaging (MRI) and compatible with malignant transformation. In this case, the only surgical option would have been a transmandibular approach, but it was considered too morbid for the patient.
Discussion
Primary lesions of the PPS are mainly benign (80% according to the 2 comprehensive reviews by Riffat et al. 2 and Kuet et al. 3), which means that the main goal of surgery is enucleation, possibly without damaging the capsule and with a minimal, if any, cuff of surrounding soft tissues. Even for primary malignant lesions, the concept of resection margins is debatable, considering the anatomy of this space, tightly enclosed by muscular and bony boundaries, and filled in with vital neurovascular structures. In this scenario, any surgery should find the appropriate balance between an adequate space for manoeuvres plus lesion extraction and preservation of intact adjoining structures, since the nature of these lesions would not justify an excessive morbidity 12. Although some authors have recently evaluated the exposure provided by each existing surgical approach to the PPS4, surgeons rarely handle the entire range of techniques and tend to rely primarily on one or 2. Ideally, one should be able to choose the best access according to the lesions’ biology and location, possibly integrating the corridors and/or increasing the space, similarly to what is nowadays known as the modular approach in oral cavity 13 or laryngeal surgery 14. Both Chu et al. 10 and Lombardi et al. 5 have proposed an algorithm in this scenario, based on the extension of the lesion, but also on preoperative (e.g. location of the internal carotid artery) and intraoperative (e.g. infiltration) findings.
Classically, the cervical or cervical-parotid approach is the most widely used (48-54%) 2,3, and is ideal for laterally and inferiorly located lesions, but it does not grant sufficient exposure of the deeper portion of the PPS, particularly in its upper third4. Hence, this surgery is typically completed with a blind finger dissection of the medial surface of the lesion, which may eventually be successful, but also associated with a considerable risk of capsule damage or fragmentation and, ultimately, tumour spillage. This technique has proven successful even in case of voluminous benign lesions 15-17 without the need for mandibulotomy to gain wider exposure. Nevertheless, none of the articles cited reports on the type of dissection of the medial portion of the lesions, nor about any capsular damage/interruption in cases of pleomorphic adenoma. Only one article states that “in nine cases margins were closed or positive due to the surgical technique of blunt dissection” 15: given that all lesions were benign, this is arguably a periphrasis for “capsule violation”, to say the least.
Conversely, the transoral approach allows better access to the medial portion of the PPS, particularly in its middle third, while it is limited when the lesion extends superiorly, inferiorly and/or laterally 4. This holds true even when the transoral approach is endoscope-assisted or robotic-assisted: although such technology has highly enhanced visualisation, overcoming the inferior and lateral limits of dissection, and expanding indications even to large or retrostyloid lesions 18,19, it is still hindered by other intrinsic limitations of a transoral route, mainly the exposure of the upper parapharyngeal space and the relationship between the lesion and major vessels 6,10. For this reason, the position and the extension of any parapharyngeal lesion, rather than its pure dimension, need to be carefully evaluated whenever an exclusive transoral approach is contemplated 20. In this regard, the role of an experienced radiologist in preoperative work-up is crucial to assess the relationship of the lesion with the surrounding structures and to anticipate any possible steric or biologic features which could complicate the surgery. To our knowledge, only Boyce et al. recommended that a transoral approach be combined with a cervicotomy in case the lesion extends closer than 10 mm to the skull base and/or laterally beyond the stylomandibular ligament 11. This is a valuable suggestion, of course, but it may be too simplistic: in fact, even in the transoral approach, finger blunt dissection may help the detachment of the lesions’ superior or lateral boundaries, especially when haptic feedback is lacking, as is the case of TORS 19,20. Moreover, in some experiences, even large tumours could be excised transorally without the need for further transcervical access 18,21. In such cases, extending the mucosal incision upward in the soft palate and/or sectioning part of the medial pterygoid muscle from pterygoid lamina may provide a wider access, without necessarily augmenting the morbidity of the procedure 18,22. In our experience, such procedures were not associated with velopharyngeal insufficiency or trismus, respectively, although they should be employed carefully and always balanced with the risk of fragmentation or subtotal removal.
Interestingly, the new Da Vinci SP (single-port) enhances the capability of exploring the surgical field thanks to its flexible optics, which can change the angle of vision from 0° to 30°, instantly, without changing the scope. Furthermore, it allows the use of a third robotic arm, which can provide constant alternating traction of the medial or lateral mucosal flap (Fig. 1), without the need to find additional space for introduction and manoeuvres.
Other authors have proposed a combined approach by means of TORS and a transcervical endoscopic-assisted access: nonetheless, indications for such combination were not so precise (“high small benign PPS tumours such as pleomorphic adenomas which are difficult to reach by blunt dissection, and difficult to visualise adequately and dissect laterally by TORS approach alone; large pleomorphic adenomas of the PPS; encapsulated carcinoma ex pleomorphic adenomas or adenocarcinomas without extracapsular extension; symptomatic PPS schwannomas”) 23.
In our opinion, it is difficult to provide exhaustive indications for a combined approach based solely on preoperative work-up 10, because intraoperative findings are crucial, in terms of the lesion’s consistency and adherence to the surrounding tissues, and because mouth opening may alter the static relationship between the lesion and the bony and muscular structures revealed at preoperative imaging. Whenever not absolutely contraindicated (e.g. trismus, unequivocal malignant infiltration of surrounding tissues, medial displacement of internal carotid artery) 10 and technically available, transoral robotic surgery should be primarily considered for lesions of the PPS, given the possibility for a finer dissection. Nonetheless, exclusive TORS is definitely not recommended if the lesion originates from or is in tight contact with the deep lobe of the parotid gland (including an hourglass-shaped extension lateral to the mandible) (Fig. 2), which would require a rather difficult transoral dissection at risk of damaging the facial nerve and the capsule, and/or the lesion’s shortest axis is larger than the interincisal gap (IIG), which would not allow for extraction from the mouth. In all other cases, even when a mass is large and possibly extends to the skull base or the masticator space, TORS has the potential to be a single procedure for removal. The transoral robotic resection is aided by wet pledgets, which allow atraumatic capsule-preserving detachment of fibrous adherences, but it may also take advantage of careful finger and/or hand instrument dissection, which is not to be demonised (Fig. 3). Such dissection may be performed even under direct visual control with loupes, after removing the robotic arms: this process, and the ensuing replacement, may be time-consuming, but the safety and effectiveness of this tactile manoeuvre make it worthwhile 20. This manoeuvre is even more reliable in robotic surgery because 3D magnified vision allows better identification of the true capsule of the mass and, consequently, of the correct plane for digital dissection. Of note, with the advent of the Da Vinci SP, replacement of the robotic arms has become easier and faster, even for inexperienced assistants.
Importantly, TORS does not limit further surgical routes whenever the parapharyngeal lesion cannot be dominated, thus it represents only one part of a modular approach.
The surgical timing of a combined approach is an important issue as well. When the lesion can only be removed through the neck, the transoral approach should be the first step, aimed at detaching the medial portion under direct visual control. Conversely, when the lesion can be delivered through the mouth, and, hence, the transcervical/transparotid access is needed to dissect the far lateral portion and can be as small as possible, the transoral approach may either precede or follow, based on the possibility of an exclusive procedure: if this is not feasible (see above), the transcervical access should be the first step, in order to maintain an aseptic technique.
The advantage of a modular approach is the possibility to increment gradually the morbidity of the whole surgery, saving a mandibulotomy for last. Of note, in case a trans-mandibular approach is a viable option, to be determined intraoperatively, but suspected on preoperative imaging (e.g. doubtful infiltration of the skull base or hypervascularisation of the mass), we recommend that surgery begin with a transcervical access and that TORS be initiated only when a mandibulotomy is excluded, in order to reduce the surgical time and, especially, to spare an unnecessary pharyngotomy with the ensuing co-morbidity.
Although reviewing the existing mandibulotomy techniques falls outside the focus of the current paper, it is worth mentioning that even the transmandibular approach can be modulated, based on the exposure gained during the surgery. Unlike other maxillo-facial colleagues, who tend to present new straightforward techniques, Kolokythas et al. proposed a rational algorithm where the transmandibular approach is anticipated but not unavoidable, and, most importantly, may consist of a single anterior (parasymphyseal) osteotomy or, when insufficient for exposure, a double osteotomy, with the latter at the level of the ramus 24. As stated by the same authors, any time a mandibular osteotomy is considered, 3 further issues need to be managed, i.e. occlusion, temporomandibular joint function, and inferior alveolar nerve sensation. These concerns should prompt a thoughtful use of any transmandibular approaches, together with a reflection on the meaning of “acceptable morbidity” 25.
In this regard, a brief remark is needed. In our opinion, the morbidity of a surgical approach, and particularly a minimally-invasive one, should be evaluated in its entirety, especially in terms of neuro-vascular complications and timing of overall recovery, rather than hospital stay or placement of a tracheal tube. That said, we probably tend to be overly cautious in terms of both airway protections and reuptake of oral feeding, even today.
Last, but not least, the modular approach to the PPS may be implemented by a further minimally-invasive corridor, i.e. the trans-nasal endoscopic route. The combination of TORS and endonasal endoscopy was first explored by Carrau et al. back in 2013 26, while Mao et al. later presented a case series (6 patients) on an endoscopic endonasal combined transoral medial approach 27. Despite minimal numbers, these experiences demonstrate that it is possible to combine the approaches successfully, and that the restricted space of manoeuvre in the upper PPS of the transoral access may be overcome by the transnasal corridor, which is well-known to grant optimal control over this region 28,29.
A few limitations of our study need to be acknowledged. This is a retrospective study of a larger series of parapharyngeal lesions (n = 109, data unpublished) treated with different techniques, and therefore we cannot draw conclusive indications on the most suitable approach, but rather present a collection of educated recommendations. A more articulated and evidence-based treatment algorithm with clinical and radiological parameters could be the focus of a future multicentric prospective study. Nevertheless, the experience of our department in TORS of the PPS is solid and, in our opinion, offers valuable ground for academic discussion and clinical improvements. Of course, we must keep in mind that this approach is not devoid of complications, particularly the risk of adenoma capsular damage or even fragmentation, and thus the risk of recurrence. Moreover, we would like to emphasise that, although the combined approach does not compromise a possible subsequent transmandibular approach, even years later, in cases of extreme necessity, it requires experience and expertise to be managed, like any surgical procedure involving the complex PPS.
Finally, we must acknowledge that robotic surgery is inevitably associated with an increased cost of intraoperative equipment, which reflects on the overall cost of the patient’s care. Nonetheless, the impact on the health system depends on several different aspects, including the treatment of early and late complications. Ideally, the use of robotic surgery should be evaluated countrywide in terms of costs and benefits, after more experience is gained, to refine indications and minimise the morbidity.
Conclusions
TORS is a viable option for lesions of the parapharyngeal space. It may be combined with an external access, i.e. transcervical and/or transparotid, or with an endonasal endoscopic route, giving rise to what may be called a “modular approach”. More invasive surgery, namely mandibular osteotomies, is not impeded, but should be kept as a last resort because of undeniable and potentially unjustified morbidity.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This work was partially funded by the Italian Ministry of Health with Ricerca Corrente and 5 × 1000 funds.
Author contributions
GP, SFZ, MA: study conception and design; FB, FC: acquisition of data; GP, CM, FR: analysis and interpretation of data; GP: drafting of manuscript; SFZ, GG, MA: critical revision and final approval.
Ethical consideration
This study was approved by the Institutional Ethics Committee of the European Institute of Oncology (approval number: 3016).
The research was conducted ethically, with all study procedures being performed in accordance with the requirements of the World Medical Association’s Declaration of Helsinki.
Written informed consent was obtained from each participant/patient for study participation and data publication.
History
Received: March 3, 2025
Accepted: August 10, 2025
Figures and tables
Figure 1. Endoscopic view of an exclusive transoral procedure with Da Vinci SP for a left parapharyngeal neurofibroma. The furthest right arm is equipped with Cadiere forceps, which pull the mucosal flap medially to widen the surgical access, while the dissection is carried out with the other two arms (Maryland forceps and electrocautery spatula).
Figure 2. CT scan axial and coronal views of a pleomorphic adenoma of the deep lobe of the left parotid gland, encroaching on the ipsilateral parapharyngeal space. Such a case is not amenable to exclusive transoral robotic surgery.
Figure 3. Endoscopic view of an exclusive transoral procedure with Da Vinci SP for a right parapharyngeal pleomorphic adenoma. Blunt dissection is carried out with wet pledgets handled by robotic arms (A), but also with finger (B) and hand-held instruments (C).
| Overall cohort (n = 43) | |
|---|---|
| Gender | |
| M | 26 (60.5%) |
| F | 17 (39.5%) |
| Median age (IQR), years | 53 (42.5-66.5) |
| Type of surgery | |
| Therapeutic | 40 (93%) |
| Diagnostic | 3 (7%) |
| Residual tumour after therapeutic surgery (n = 9) | |
| Yes | 2 (5%) |
| No | 38 (95%) |
| Type of combined procedure (n = 9) | |
| Transoral + transcervical | 6 (66.7%) |
| Transcervical + transoral | 2 (22.2%) |
| Transoral + transparotid | 0 (0%) |
| Transparotid + transoral | 1 (11.1%) |
| Final histology | |
| Pleomorphic adenoma | 23 (53.5%) |
| Schwannoma | 3 (7%) |
| Carcinoma ex pleomorphic adenoma | 3 (7%) |
| Metastatic papillary carcinoma | 2 (4.7%) |
| Myoepithelioma | 2 (4.7%) |
| Adenoid cystic carcinoma | 1 (2.3%) |
| Mucoepidermoid carcinoma* | 1 (2.3%) |
| Plasmocytoma | 1 (2.3%) |
| Well-differentiated liposarcoma | 1 (2.3%) |
| Oncocytoma | 1 (2.3%) |
| Rhabdomyoma | 1 (2.3%) |
| Neurofibroma | 1 (2.3%) |
| Cavernous haemangioma | 1 (2.3%) |
| Angiolipoma | 1 (2.3%) |
| Branchial cyst | 1 (2.3%) |
| IQR: interquartile range; * histology on diagnostic procedures. | |
References
- Prasad S, Piccirillo E, Chovanec M. Lateral skull base approaches in the management of benign parapharyngeal space tumors. Auris Nasus Larynx. 2015;42:189-198. doi:https://doi.org/10.1016/j.anl.2014.09.002
- Riffat F, Dwivedi R, Palme C. A systematic review of 1143 parapharyngeal space tumors reported over 20 years. Oral Oncol. 2014;50:421-430. doi:https://doi.org/10.1016/j.oraloncology.2014.02.007
- Kuet M, Kasbekar A, Masterson L. Management of tumors arising from the parapharyngeal space: a systematic review of 1,293 cases reported over 25 years. Laryngoscope. 2015;125:1372-1381. doi:https://doi.org/10.1002/lary.25077
- Ferrari M, Schreiber A, Mattavelli D. Surgical anatomy of the parapharyngeal space: multiperspective, quantification-based study. Head Neck. 2019;41:642-656. doi:https://doi.org/10.1002/hed.25378
- Lombardi D, Ferrari M, Paderno A. Selection of the surgical approach for lesions with parapharyngeal space involvement: a single-center experience on 153 cases. Oral Oncol. 2020;109. doi:https://doi.org/10.1016/j.oraloncology.2020.104872
- Chan J, Tsang R, Eisele D. Transoral robotic surgery of the parapharyngeal space: a case series and systematic review. Head Neck. 2015;37:293-298. doi:https://doi.org/10.1002/hed.23557
- De Virgilio A, Costantino A, Mercante G. Trans-oral robotic surgery in the management of parapharyngeal space tumors: a systematic review. Oral Oncol. 2020;103. doi:https://doi.org/10.1016/j.oraloncology.2020.104581
- Zhu X, Shi X, Zhou L. Trends in the surgical management of parapharyngeal space tumors: a single-center retrospective analysis. Eur J Surg Oncol. 2023;49:47-54. doi:https://doi.org/10.1016/j.ejso.2022.08.016
- Chu F, De Berardinis R, Tagliabue M. The role of transoral robotic surgery for parapharyngeal space: experience of a tertiary center. J Craniofac Surg. 2020;31:117-120. doi:https://doi.org/10.1097/SCS.0000000000005912
- Chu F, Tagliabue M, Giugliano G. From transmandibular to transoral robotic approach for parapharyngeal space tumors. Am J Otolaryngol. 2017;38:375-379. doi:https://doi.org/10.1016/j.amjoto.2017.03.004
- Boyce B, Curry J, Luginbuhl A. Transoral robotic approach to parapharyngeal space tumors: case series and technical limitations. Laryngoscope. 2016;126:1776-1782. doi:https://doi.org/10.1002/lary.25929
- López F, Suárez C, Vander Poorten V. Contemporary management of primary parapharyngeal space tumors. Head Neck. 2019;41:522-535. doi:https://doi.org/10.1002/hed.25439
- Gazzini L, Dallari V, Caselli A. Modular anatomic approach to oral tongue carcinoma: functional outcomes and quality of life. Acta Otorhinolaryngol Ital. 2024;44:285-295. doi:https://doi.org/10.14639/0392-100X-N3041
- Crosetti E, Fantini M, Bertotto I. Current status of partial laryngeal surgery for advanced laryngeal cancer: when and why?. Curr Oncol Rep. 2024;26:614-624. doi:https://doi.org/10.1007/s11912-024-01516-7
- Presutti L, Molteni G, Malvè L. Parapharyngeal space tumors without mandibulotomy: our experience. Eur Arch Otorhinolaryngol. 2012;269:265-273. doi:https://doi.org/10.1007/s00405-011-1594-y
- Basaran B, Polat B, Unsaler S. Parapharyngeal space tumours: the efficiency of a transcervical approach without mandibulotomy through review of 44 cases. Acta Otorhinolaryngol Ital. 2014;34:310-316.
- Wani A, Khan R, Rehman A. Conservative lateral approach for pleomorphic adenomas of parotid gland involving the parapharyngeal space – A case series. Indian J Otolaryngol Head Neck Surg. 2022;74:5800-5805. doi:https://doi.org/10.1007/s12070-021-02409-y
- Ansarin M, Tagliabue M, Chu F. Transoral robotic surgery in retrostyloid parapharyngeal space schwannomas. Case Rep Otolaryngol. 2014;2014. doi:https://doi.org/10.1155/2014/296025
- O’Malley B, Quon H, Leonhardt F. Transoral robotic surgery for parapharyngeal space tumors. ORL J Otorhinolaryngol Relat Spec. 2010;72:332-336. doi:https://doi.org/10.1159/000320596
- Larson A, Ryan W. Transoral excision of parapharyngeal space tumors. Otolaryngol Clin North Am. 2021;54:531-541. doi:https://doi.org/10.1016/j.otc.2021.03.001
- Panda S, Sikka K, Thakar A. Transoral robotic surgery for the parapharyngeal space: expanding the transoral corridor. J Robot Surg. 2020;14:61-67. doi:https://doi.org/10.1007/s11701-019-00932-3
- Tsai C, Wu S, Lin S. Reducing trismus after surgery and radiotherapy in oral cancer patients: results of alternative operation versus traditional operation. J Oral Maxillofac Surg. 2016;74:1072-1083. doi:https://doi.org/10.1016/j.joms.2015.11.034
- Duek I, Sviri G, Billan S. Minimally invasive surgery for resection of parapharyngeal space tumors. J Neurol Surg B Skull Base. 2018;79:250-256. doi:https://doi.org/10.1055/s-0037-1607315
- Kolokythas A, Eisele D, El-Sayed I. Mandibular osteotomies for access to select parapharyngeal space neoplasms. Head Neck. 2009;31:102-110. doi:https://doi.org/10.1002/hed.20934
- Schlieve T, Carlson E, Freeman M. The double mandibular osteotomy for vascular and tumor surgery of the parapharyngeal space. J Oral Maxillofac Surg. 2017;75:1046-1061. doi:https://doi.org/10.1016/j.joms.2016.11.003
- Carrau R, Prevedello D, de Lara D. Combined transoral robotic surgery and endoscopic endonasal approach for the resection of extensive malignancies of the skull base. Head Neck. 2013;35:E351-E358. doi:https://doi.org/10.1002/hed.23238
- Mao S, Tang R, Gu Y. Endoscopic endonasal combined transoral medial approach to the nasopharynx, parapharyngeal space, and jugular foramen. Head Neck. 2024;46:485-491. doi:https://doi.org/10.1002/hed.27596
- Battaglia P, Turri-Zanoni M, Dallan I. Endoscopic endonasal transpterygoid transmaxillary approach to the infratemporal and upper parapharyngeal tumors. Otolaryngol Head Neck Surg. 2014;150:696-702. doi:https://doi.org/10.1177/0194599813520290
- Liu Q, Wang H, Zhao W. Endoscopic transnasal transmaxillary approach to the upper parapharyngeal space and the skull base. Eur Arch Otorhinolaryngol. 2020;277:801-807. doi:https://doi.org/10.1007/s00405-019-05761-6
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 350 times
- PDF downloaded - 70 times