Audiology
Vol. 46: Issue 2 - April 2026
Assessment of language development in children with prelingual single-sided deafness
Authors
Dorota Pastuszak
 , Anita Obrycka
, Henryk Skarżyński
, Piotr Henryk Skarżyński
, Anita Obrycka
, Henryk Skarżyński
, Piotr Henryk Skarżyński
Summary
Cover Image
Objectives. To assess the development of receptive and expressive language skills in children who had prelingual single-sided deafness (SSD).
Materials and methods. Fifty children diagnosed with SSD at the Institute of Physiology and Pathology of Hearing in Warsaw/Kajetany, Poland were included in the study. Receptive and expressive language skills were examined using a norm-referenced test, the Child Speech Therapy Assessment Cards (CSTAC).
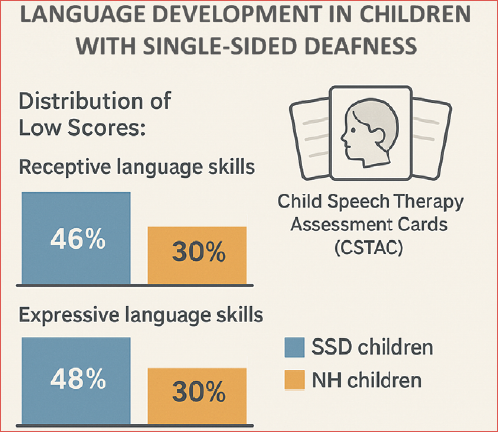
Results. In the test of receptive language skills, 46% of children with SSD received low scores, while 48% recorded low scores in the test of expressive language skills. Among children with normal hearing, the expected percentage of low scores is 30.8% for both receptive and expressive skills. Children with SSD demonstrated a significantly higher proportion of low scores in both receptive (χ2 [2, n = 50] = 19.66; p < .001; V = 0.63) and expressive (χ2 [2, n = 50] = 22.64; p < 0.001; V = 0.67) language skills compared to their normal-hearing peers.
Conclusions. The results showed that children with SSD are at risk of language delays. To minimise the potential consequences of such delays, appropriate early intervention – together with parental education, speech-language therapy, auditory training, and monitoring of language development – should be implemented.
Introduction
Single-sided deafness (SSD) is a condition where a patient has severe or profound hearing loss (> 90 dB HL) in one ear and normal hearing (NH) or mild hearing loss (≤ 30 dB HL) in the other 1-3. For many years, SSD has been considered a non-disabling hearing loss 4.
A growing body of research shows that children with SSD are at risk of school underachievement, emotional difficulties, and problems with complex cognitive skills 5-8. It has been shown that SSD children have difficulty with auditory attention, especially in recognising features of sounds, speech, and auditory memory, all of which are critical for language development. Additionally, children with SSD experience listening fatigue which leads to poorer sentence recognition and lower processing speed, all of which may impair learning 9,10. Some 22-35% of children with SSD are not promoted to the next class, and 12-41% need additional educational support 4,11,12. Often, children with SSD feel less self-confident in noisy settings, which can lead to avoidance of social contacts and meeting up with peers 5,13.
The risks of school underachievement in children with SSD, as well as their more likely emotional and psychosocial problems, often relate to a lack of binaural hearing 12. Having 2 ears with normal hearing guides appropriate auditory development, especially in terms of sound localisation and ability to segregate sounds from noise. Lack of those abilities in children with SSD not only affects incidental language learning 7,14, but also hampers effective communication, especially in background noise and under adverse listening conditions 15. As a result, the development of language and communication skills in children with prelingual SSD may be delayed 16,17.
There have only been a few reports on the effects of SSD on language development in children 7,16,18-20. Some of them reported delays in language development in SSD compared to NH children specifically in both receptive and expressive skills 7,19,20, while others report delays in only one area 16. There is no general agreement about whether the observed delays resolve with age 16,20. Moreover, those studies focused on different age groups: 1-3 18, 2-5 16, 6-12 19, 5-15 7, and 12-17 years 20. Most authors advocate further research on language development of children with SSD, with one important aim being to improve family counselling and share decision-making about possible interventions 7,19,20.
When looking at possible factors associated with language development in SSD children, authors pointed at maternal education, birth order, family income, gender, and the side of deafness 16,19,20. Exploring the factors related to language outcomes in SSD children can assist in determining the risk of delays in language skills development and point to appropriate treatment and therapy 7,16.
Given above considerations, the aim of this study was to examine the development of receptive and expressive language skills in children with prelingual SSD. We also explored factors related to language development such as gender, side of deafness, age at evaluation, and the onset and aetiology of deafness.
Materials and methods
Subjects
Fifty children, aged from 4 months to 9 years (mean, 3 years; SD = 2.4) were included in the study. They were diagnosed with SSD and referred to the Institute of Physiology and Pathology of Hearing in Warsaw/Kajetany, Poland, between September 2020 and November 2023. All patients underwent a medical examination and were consulted with a psychologist. Their behaviour during the examination, combined with results from psychological tests such as the Bayley Scales of Infant and Toddler Development, Fourth Edition (Bayley-4), and the Wechsler Preschool and Primary Scale of Intelligence (WPPSI-IV), confirmed typical development. None of the children had comorbidities. Hearing thresholds were evaluated with auditory brainstem response test or with pure-tone audiometry.
Based on the results of newborns hearing screening (NHS), congenital SSD was found in 40 of them. In 10 children, the precise date of onset of acquired SSD could not be identified; although hearing loss was diagnosed at ages of 1 to 6 years, most parents reported they had noticed some symptoms at earlier times. Within the study group, 27 children attended kindergarten or school, and 25 children participated in rehabilitation sessions. None of the children in the group used hearing technologies. Details of the study group are given in Table I.
Language development evaluation
Receptive and expressive language skills were examined using the Child Speech Therapy Assessment Cards (CSTAC). Most speech and language assessment tools available in Poland are proprietary instruments that lack standardisation. In contrast, CSTAC is a norm-referenced test designed for children from 1 month to 9 years and has been developed, standardised, and normalised in a population of Polish children 21. The test includes normative tables, enabling objective comparisons of a child’s performance with age-specific groups. Additionally, most existing tools assess only isolated areas, such as articulation, whereas CSTAC provides a comprehensive evaluation of language development. CSTAC is tailored to 12 age groups, with separate tasks designed for each group. Unlike most tools – which typically begin at ages 3-4 or apply the same tasks across broad age ranges – only CSTAC enables precise assessment from infancy. It is recommended by the Polish Association of Speech Therapists (Polski Związek Logopedów, PZL) as a reliable, valid, and diagnostically sensitive tool that aligns with current medical, psychological, and educational standards.
CSTAC tests have been developed for 12 age groups covering 4 developmental periods:
- Infancy (1st month to the end of the 11th month), with separate tests for 1-4, 5-8, and 9-11 months;
- Post-infantile (12 months to the end of 35 months), with separate tests for 12-17, 18-23, and 24-35 months;
- Pre-school (3-6 years), with separate tests for 3, 4, and 5 years;
- Elementary school (6-9 years), with separate tests for 6, 7, and 8-9 years.
Based on performance in set tasks, CSTAC determines vocabulary and grammatical constructions used by children in particular age groups. For receptive language, it starts from simple tasks in infancy and ends with complex tasks in school children. The following skills are tested: reaction to speech, reaction to play and imitation, eye contact, communication dyad/triad, understanding utterances (nouns, verbs, adjectives, adverbs), carrying out simple/complex commands, noticing illogicality, categorisation, and time consequences. In the area of expressive language, speech production ability is tested, first with cooing and babbling, then baby talk, vocalisations, alternation in conversation, producing speech sounds, first words, combining words, and ending with the breadth of vocabulary (nouns, verbs, adjectives, adverbs), declination of nouns, conjugation of verbs, giving definitions, and telling a story. Testing with CSTAC provides both quantitative and partially qualitative results. A speech therapist can then make a diagnosis with reference to the ICD-10 classification, and describe the results in terms of age group norms. The examination should be performed by a certified speech therapist with appropriate training.
Normalisation of CSTAC was done in a group of 1,083 normally developing children aged from 1 month to 9 years 21. Normalisation allows an individual’s performance to be ranked in relation to others in that population. CSTAC has been normalised using a sten scoring system from 1 to 10 (“Standard Ten score”). The scale divides receptive and expressive language skills of normal developing children into 3 categories of sten scores: 1 to 4 (30.8% of children) indicate a low level of the tested feature, 5 and 6 (38.3% of children) indicate an average level, while from 7 to 10 (30.8% of children) indicate a high level of the tested trait.
Scoring of a child is based on a zero/one system: a child will either complete the task correctly and receive 1 point, otherwise receive 0 points. Sums of separate raw scores for receptive and expressive language skills are converted into one of 3 categories – low, average, or high – according to a key based on normalised sten scores.
Statistical analysis
The distributions of low, average, and high scores in the study group and in the group of children developing normally were compared using a chi-square test. The chi-square test was also used to examine the relation between receptive and expressive language skills and selected factors: gender, side of deafness, age (below 3 vs 3-9 years), onset of deafness, and aetiology. In the case of expected counts less than 5 we used Yates’s correction to prevent overestimating the statistical significance of small data. The level of significance was set at α = 0.05.
Results
The distribution of low, average, and high scores for receptive and expressive language skills in the study group are presented in Figure 1. For receptive language skills, we found that 46% of children had low scores, 52% had average scores, and 2% had high scores. For expressive skills, the corresponding numbers were 48% low scores, 52% average, and 0% high. In comparison, for children developing normally, and according to the definition of the sten scores used for CSTAC normalisation, 30.8% of children receive low scores, 38.3% average, and 30.8% high (on both assessments). The chi-square test for a one-way table revealed that there was a significant difference between the distribution of scores for SSD children and those for normally developing children: for receptive language skills χ2 (2, n = 50) = 19.66; p < 0.001; V = 0.63 and for expressive language skills χ2 (2, n = 50) = 22.64; p < 0.001; V = 0.67. In both tests, the group of children with SSD had significantly higher percentages of low scores compared with normally developing children (Cover figure).
The distribution of receptive and expressive language skills scores in SSD children are shown in Figure 2 according to the factors of gender, side of deafness, age at evaluation, and onset of deafness. Because only one child achieved a high score in the receptive skills assessment, and none in the expressive skills evaluation, to compare groups we pooled average and high scores. A chi-square test of independence showed (Fig. 2A) that, for receptive language, the distribution of scores in both tests did not differ by sex (χ2 (1, n = 50) = 0.21; p = 0.64; φ = -0.07). A similar result held for expressive language (χ2 (1, n = 50) = 0.85; p = 0.36; φ = 0.13). Figure 2B shows that side of deafness was also not a factor related to receptive language skills (χ2 [1, n = 50] = 0.25; p = 0.61; φ = 0.07) or expressive language skills (χ2 [1, n = 50] = 0.79; p = 0.37; φ = -0.13). As shown in Figure 2D, the chi-square test with Yates’s correction showed that there was no significant difference between the distribution of scores in children with congenital and acquired onset of deafness in receptive language skills scores χ2 ([1, n = 50] = 2.22; p = 0.14; φ = 0.23) nor in expressive language skills (χ2 [1, n = 50] = 0.05; p = 0.83; φ = 0.08).
Turning to significant differences, receptive language skills in terms of age resulted in χ2(1, n = 50) = 4.34; p = 0.04; φ = 0.30, suggesting a statistically significant difference in the distribution of scores between SSD children aged up to 3 years (infants and post-infant children) and those aged 3 to 9 years (pre-school and elementary school children). In younger children, the proportion of low scores was significantly higher than in older children. Similarly, among younger children the proportion of low scores for the expressive language test was significantly higher than in older children (χ2 [(1, n = 50)] = 5.48; p = 0.02; φ = 0.33), as shown in Figure 2C.
Additionally, we tested whether the distribution of scores for both age groups of SSD children followed the distribution of sten scores of children developing normally. Chi-square tests for a one-way table revealed significant differences. For those aged up to 3 years, the results of the receptive language test gave χ2 (2, n = 29) = 16.27; p < 0.001; V = 0.75, and for expressive language χ2 (2, n = 29) = 18.11; p < 0.001; V = 0.79. Similarly, for children aged 3 to 9 years, the receptive language test gave χ2 (2, n = 21) = 9.08, p = 0.01; V = 0.66; and the expressive language test gave χ2 (2, n = 21) = 12.53, p = 0.002; V = 0.77.
Figure 3 shows the distribution of scores for receptive and expressive language skills in relation to the aetiology of SSD. A formal analysis could not be performed because of the high number of cases (n = 27) of unknown SSD aetiology and the relatively small number of observations in the remaining 3 categories (7, congenital cytomegalovirus; 11, inner ear pathology; 5, virus infection). The large disparity in numbers between observations in the individual categories violates the assumptions of the chi-square test, which requires that expected frequencies should be 5 or more in at least 80% of the cells. Nevertheless, there was a trend towards more low scores in the SSD group that was caused by congenital cytomegalovirus (where the percentages were 71% for receptive skills and 86% for expressive skills).
Discussion
Limited information exists about the effect of SSD on language development. The few studies conducted so far indicate delays in language development in children with SSD compared to their normal hearing peers 7,19,20. At the same time, some authors report an expressive language deficit but no receptive deficit 16, and some have found, without formal analysis, lower scores in SSD children compared to NH children 18. The publications in this area are not only limited but differ in age groupings. Moreover, it is not clear whether other factors apart from SSD are associated with language development. Our study sought to complement existing knowledge in this area, so we decided to focus on receptive and expressive language skills in children with untreated prelingual SSD. We tested young children (before the age of 3) as well as children from 3 to 9 years, and explored factors related to language development.
Despite such a large age range of tested children, the assessment test used in the study allowed reliable analyses to be conducted. CSTAC was prepared for different age groups and normalised separately in each group using the sten scoring system. Thus, regardless of age, the results for each tested child could be classified into one of 3 categories. This allowed us to analyse the frequency of results in relation to NH children and perform between-group comparisons. Our results clearly point towards lower scores in receptive and expressive language skills for SSD children compared to NH children.
Due to differences in methods and tests used in previous studies, making detailed or direct comparisons was not feasible. Therefore, we compared our results with prior works in a more general manner. Our results generally confirm previous findings 7,16,18-20.
Two of those previous studies 16,18 looked at language skills (receptive and expressive) among young children with congenital SSD. Arras et al. 16 looked at 16 children with SSD and compared their results with a group of normal hearing peers and a group of SSD children treated with a cochlear implant (CI). All children were aged 2 to 5 years. The results showed that children with SSD had worse grammar scores (expressive skills) than the NH group and the CI group, but there were no differences between the groups in terms of receptive language skills. Sangen et al. 18 tested 12 toddlers (1-3 years old) and found that half of them with untreated SSD performed worse that NH children in terms of both receptive and expressive language. In our study, the proportion of low scores was even higher, so that in the subgroup of 39 SSD children aged 4-35 months, 59% had low scores in receptive language development and 62% had low scores in expressive language development. Thus, the percentage of low scores in SSD children was double that of NH children.
A similar to our study, negative effect of unilateral hearing loss (UHL) on language skills was found in a study by Lieu et al. 19 involving elementary school children. The authors examined children aged 6-12 years, including 74 with NH and 74 with different levels of UHL, of whom 44 had SSD. The results showed that children with UHL had significantly worse language comprehension scores, oral expression, and oral composite scores than their peers with NH. In a related study, Sangen et al. 7 looked at the effect of SSD on 21 children 5-15 years old and found differences in language and auditory skills between the SSD and NH children. The lower performance stood out in the areas of morphology, syntax, and vocabulary. In our study, in the subgroup of 29 children aged 3-9 years, 29% received low scores in receptive and expressive language. That percentage is comparable with the proportion of low scores in NH children (30.8%). To complete the picture, we also observed a higher proportion of average scores in this group (66.7% in receptive and 71.4% in expressive skills assessment). At the other end of the scale, no high scores for expressive skills were observed among our SSD children aged 3-9 years, and for receptive skills only one child had a high score (whereas in NH children the rate of high scores is 30.8%).
The higher proportion of low scores for receptive and expressive skills in SSD children than in NH children can be attributed to impaired speech perception in the presence of noise due to their lack of binaural hearing 22. It has been demonstrated that background speech disrupts memory, understanding oral instructions, and categorisation of speech sounds, all of which are crucial for language development 23,24. Considering that competing noises at home, kindergarten, or school negatively impacts language development in normally developing children, we can expect that this effect will be stronger in SSD children.
Among factors associated with language development in children with SSD we looked at gender, side of deafness, age, onset of deafness, and etiology. We did not find any differences in the distribution of scores between boys and girls or between left and right side of deafness. These findings concerning gender and side of deafness are in line with Lieu et al. 19 and Fischer and Lieu 20.
In contrast, age was found to be a major factor in affecting score distribution. In our study the proportion of low scores in children below the age of 3 years (59% and 62% in receptive and expressive language) was significantly greater than in children 3-9 years old (where the figures were 29% in both areas). However, we did see a lower proportion of low language development scores in older children, but the older group still performed worse than their NH peers. Our results align with previous findings indicating that children with SSD have lower language scores than their NH peers across different age groups 7,16,18-20.
The smaller proportion of low scores in children aged 3-9 years compared to children below 3 years might be associated with the beginning of education. When children begin pre-school (usually at age 3) or primary school they are usually evaluated by a speech therapist and undergo rehabilitation if required. The rehabilitation and therapy of young SSD children probably helps them improve their scores, but they were still unable to catch up with their NH peers. Another interpretation is that older children develop compensatory strategies in order to communicate in a noisy environment, e.g. by positioning the ear with normal hearing towards the speaker 25. The smaller proportion of low scores in older children may also be related to their parents’ greater experience in creating favourable acoustic environments for conversing with their SSD child, one free of competing noise.
In the study by Lieu et al. 19, the age at which unilateral hearing loss was identified was included as a factor in their language development model. In our study there were no differences in distribution of scores between those with congenital and acquired SSD. This may be because our study group acquired hearing loss early, in the prelingual stage of language development. Moreover, the group of participating children was rather homogeneous with regard to the onset of SSD, with 80% of children having congenital SSD. Due to imbalance between the groups in terms of onset of deafness, differences between them may not be detected.
The relationship between the aetiology of SSD and a child’s language development has not yet been determined, although the need for such an investigation was indicated by Sangen et al. 18 and Lieu et al. 19. We attempted to investigate this factor in the present work, although we were hampered because in 54% of cases the cause of hearing loss was unable to be determined, despite imaging and a detailed interview with the parents. The high percentage of cases of unknown etiology did not allow a formal analysis to be conducted. Nevertheless, we did observe that, compared to other aetiologies, there was a trend towards larger percentages of low scores among individuals with SSD caused by congenital CMV. We failed to see any other disabilities in this group of patients, although they might still be at risk of later neurological and developmental problems. The question of how aetiology relates to language development in children with SSD remains open and requires further investigation.
This study has certain limitations that need to be addressed. Although there was a large cohort of 50 SSD children from 4 months to 9 years of age, our study used a cross-sectional design, which meant it was impossible to perform longitudinal follow-ups and repeated measures. We are therefore unable to answer the question of whether the higher incidence of low scores in younger children resolves with age. To overcome this problem future prospective longitudinal studies are needed.
Secondly, there was a considerable imbalance between the groups regarding onset of SSD. In 80% of children SSD was detected at NHS, but in 20% the precise time of acquiring SSD could not be determined, although we could ascertain that a diagnosis was made at the prelingual stage. Therefore, it remains unclear whether the lack of difference in score distributions between children with congenital and acquired SSD is due to both groups being in the prelingual stage of language development, or whether it is due to an imbalance in the size of the groups which limited the power of the statistical test used.
The third limitation is the large number of children with unknown aetiology of SSD. The high fraction of cases of unknown aetiology compared to other etiologies did not allow us to conduct a formal analysis. We could only report a trend towards higher rate of low scores among individuals with SSD caused by congenital CMV compared to other etiologies. Although determining the cause of SSD is challenging, future prospective studies with a strong focus on aetiology might overcome this limitation.
The fourth limitation concerns the participation of children from the study group in rehabilitation sessions. Half of the group attended such sessions, primarily in kindergarten or school. However, we were unable to control for the duration of their participation in the rehabilitation programme or the intensity of these sessions. Consequently, the results may be biased towards better scores, as half of the children received some form of intervention through rehabilitation. In this context, the shift toward low scores is even more striking.
Conclusions
This study has shown that children with single-sided deafness are at risk of language delays. To minimise the potential consequences of such delays, appropriate early intervention, – together with parental education, speech-language therapy, auditory training, and monitoring of language development – should be implemented. These findings underscore the need for further prospective and interventional studies to better understand the impact of single-sided deafness and its aetiology on language development and to evaluate the effectiveness of potential therapeutic strategies.
Acknowledgments
The authors would like to thank Andrew Bell for his comments on earlier versions of the manuscript.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
DP: conceptualization, methodology, investigation, data curation, writing - original draft, writing - review & editing;
AO: methodology, formal analysis, visualization, writing - original draft, writing - review & editing; HS: resources, supervision, writing - review & editing; PHS: resources, methodology, investigation, supervision, writing - review & editing. All authors have read and agreed to the published version of the manuscript.
Ethical consideration
This is a retrospective study on patients’ records. This study was approved by the Ethics Committee of the Institute of Physiology and Pathology of Hearing, Warsaw, Poland (IFPS:KB/Statement 7/2022). The research was conducted ethically with all study procedures being performed in accordance with the requirements of the World Medical Association’s Declaration of Helsinki.
History
Received: April 3, 2025
Accepted: September 4, 2025
Figures and tables
Figure 1. The distribution of low, average, and high scores for receptive and expressive language skills in the study group.
Figure 2. Distribution of scores for receptive and expressive language skills in terms of A) gender; B) side of the deafness; C) age at evaluation, and D) onset of deafness.
Figure 3. Score distributions for receptive and expressive language skills in terms of SSD aetiology. cCMV: congenital cytomegalovirus; IEP: inner ear pathology (including cochlear nerve deficiency, inner ear malformations, and enlarged vestibular aqueduct).
| N | % | |
|---|---|---|
| Gender | ||
| Female | 20 | 40 |
| Male | 30 | 60 |
| Side of deafness | ||
| Right | 22 | 44 |
| Left | 28 | 56 |
| Type of deafness | ||
| Acquired | 10 | 20 |
| Congenital | 40 | 80 |
| Aetiology | ||
| Congenital cytomegalovirus | 7 | 14 |
| Cochlear nerve hypoplasia/aplasia | 8 | 16 |
| Unilateral absence of the round window | 1 | 2 |
| Bilateral incomplete partition type II | 1 | 2 |
| Enlarged vestibular aqueduct in deaf ear, mildly enlarged in NH ear | 1 | 2 |
| Virus infection | 5 | 10 |
| Unknown | 27 | 54 |
| Audiological tests | ||
| Auditory brainstem response | 41 | 82 |
| Pure tone audiometry | 37 | 74 |
| Speech audiometry | 4 | 8 |
| Tympanometry and acoustic reflex thresholds | 50 | 100 |
| Transiently evoked otoacoustic emission (TEOAE) | 50 | 100 |
References
- Deep N, Gordon S, Shapiro W. Cochlear implantation in children with single-sided deafness. Laryngoscope. 2021;131:E271-E277. doi:https://doi.org/10.1002/lary.28561
- Lorens A, Kruszyńska M, Obrycka A. Binaural advantages in using a cochlear implant for adults with profound unilateral hearing loss. Acta Otolaryngol. 2019;139:153-161. doi:https://doi.org/10.1080/00016489.2018.1535190
- Skarzynski H, Lorens A, Kruszynska M. The hearing benefit of cochlear implantation for individuals with unilateral hearing loss, but no tinnitus. Acta Otolaryngol. 2017;137:723-729. doi:https://doi.org/10.1080/00016489.2016.1274427
- Bess F, Tharpe A. Unilateral hearing impairment in children. Pediatrics. 1984;74:206-216. doi:https://doi.org/10.1542/peds.74.2.206
- Arras T, Boudewyns A, Swinnen F. Longitudinal auditory data of children with prelingual single-sided deafness managed with early cochlear implantation. Sci Rep. 2022;12. doi:https://doi.org/10.1038/s41598-022-13247-5
- Lieu J. Permanent Unilateral Hearing Loss (UHL) and childhood development. Curr Otorhinolaryngol Rep. 2018;6:74-81. doi:https://doi.org/10.1007/s40136-018-0185-5
- Sangen A, Royackers L, Desloovere C. Single-sided deafness affects language and auditory development – A case-control study. Clin Otolaryngol. 2017;42:979-987. doi:https://doi.org/10.1111/coa.12826
- van Wieringen A, Boudewyns A, Sangen A. Unilateral congenital hearing loss in children: challenges and potentials. Hearing Res. 2019;372:29-41. doi:https://doi.org/10.1016/j.heares.2018.01.010
- Bakkum K, Teunissen E, Janssen A. Subjective fatigue in children with unaided and aided unilateral hearing loss. Laryngoscope. 2023;133:189-198. doi:https://doi.org/10.1002/lary.30104
- McGarrigle R, Gustafson S, Hornsby B. Behavioral measures of listening effort in school-age children: examining the effects of signal-to-noise ratio, hearing loss, and amplification. Ear Hear. 2019;40:381-392. doi:https://doi.org/10.1097/AUD.0000000000000623
- Bovo R, Martini A, Agnoletto M. Auditory and academic performance of children with unilateral hearing loss. Scand Audiol Suppl. 1988;30:71-74.
- Lieu J. Speech-language and educational consequences of unilateral hearing loss in children. Arch Otolaryngol Head Neck Surg. 2004;130. doi:https://doi.org/10.1001/archotol.130.5.524
- Liwo H. Cochlear implant as an important factor of the development of prosodic features in prelingually deaf children under 2 years of age. J Hear Sci. 2011;1:73-75.
- Cordeiro F, Weber MPV de M. Assessment of learning disorders using the frequency following response: systematic review. J Hear Sci. 2020;10:9-18. doi:https://doi.org/10.17430/JHS.2020.10.3.1
- Ramos Macías Á, Borkoski-Barreiro S, Falcón González J. AHL, SSD and bimodal CI results in children. Eur Ann Otorhinolaryngol Head Neck Dis. 2016;133:S15-S20. doi:https://doi.org/10.1016/j.anorl.2016.04.017
- Arras T, Boudewyns A, Dhooge I. Assessment of receptive and expressive language skills among young children with prelingual single-sided deafness managed with early cochlear implantation. JAMA Netw Open. 2021;4. doi:https://doi.org/10.1001/jamanetworkopen.2021.22591
- Pastuszak D, Obrycka A, Skarżyński P. Skuteczność stosowania implantu ślimakowego u dzieci z jednostronną głuchotą – przegląd i charakterystyka wybranych publikacji. Now Audiofonol. 2024;13:9-20. doi:https://doi.org/10.17431/na/170895
- Sangen A, Dierckx A, Boudewyns A. Longitudinal linguistic outcomes of toddlers with congenital single-sided deafness – Six with and twelve without cochlear implant and nineteen normal hearing peers. Clin Otolaryngol. 2019;44:671-676. doi:https://doi.org/10.1111/coa.13347
- Lieu J, Tye-Murray N, Karzon R. Unilateral hearing loss is associated with worse speech-language scores in children. Pediatrics. 2010;125:E1348-E1355. doi:https://doi.org/10.1542/peds.2009-2448
- Fischer C, Lieu J. Unilateral hearing loss is associated with a negative effect on language scores in adolescents. Int J Pediatr Otorhinolaryngol. 2014;78:1611-1617. doi:https://doi.org/10.1016/j.ijporl.2014.07.005
- Gruba J. Karty Oceny Logopedycznej Dziecka: Karty Oceny Logopedycznej Dziecka: Podręcznik. Gliwice: Wydawnictwo Komlogo. Wydanie 1. Komlogo; 2018.
- Akeroyd M. The psychoacoustics of binaural hearing: La psicoacústica de la audición binaural. Int J Audiol. 2006;45:S25-S33. doi:https://doi.org/10.1080/14992020600782626
- Klatte M, Meis M, Sukowski H. Effects of irrelevant speech and traffic noise on speech perception and cognitive performance in elementary school children. Noise Health. 2007;9. doi:https://doi.org/10.4103/1463-1741.36982
- Koeritzer M, Rogers C, Van Engen K. The impact of age, background noise, semantic ambiguity, and hearing loss on recognition memory for spoken sentences. J Speech Lang Hear Res. 2018;61:740-751. doi:https://doi.org/10.1044/2017_JSLHR-H-17-0077
- Lucas L, Kitterick P, . The psychological and social consequences of single-sided deafness in adulthood. Int J Audiol. 2018;57:21-30. doi:https://doi.org/10.1080/14992027.2017.1398420
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 633 times
- PDF downloaded - 135 times