Head and neck
Vol. 46: Issue 3 - June 2026
A hidden diagnosis in the tonsil: recognising and differentiating intratonsillar abscess
Authors
Kadir Sinasi Bulut
 , Fatih Gul
, Ali Ozturk
, Tuba Saadet Deveci Bulut
, Serkan Serifler
, Burak Celik
, Mehmet Ali Babademez
, Fatih Gul
, Ali Ozturk
, Tuba Saadet Deveci Bulut
, Serkan Serifler
, Burak Celik
, Mehmet Ali Babademez
Summary
Cover Image
Objective. Peritonsillar abscess (PTA) and intratonsillar abscess (ITA) are distinct entities, but the latter is often overlooked due to its rarity and diagnostic difficulty. This study compares their clinical, laboratory, and microbiological profiles to identify distinguishing features.
Methods. This single-centre retrospective study included 367 patients diagnosed with PTA (n = 311) or ITA (n = 56) between 2019 and 2025. Demographics, symptoms, laboratory markers (e.g., white blood cells [WBC], neutrophils, lymphocytes, large unstained cells [LUC], C-reactive protein, sodium, neutrophil-to-lymphocyte ratio, systemic immune-inflammation index, and platelet-to-WBC ratio [PWR]), culture results, imaging, drainage outcomes, and hospital stay were analysed comparatively.
Results. PTA cases showed significantly higher WBC, neutrophil counts, and drainage volumes, with 80.8% drainage success versus 19.1% in ITA (p < 0.001). LUC and PWR were significantly elevated in ITA, suggesting a lymphocyte-dominant response. Fever was more frequent in ITA, while trismus and local spread were more characteristic of PTA.
Conclusions. ITA typically presents with smaller abscesses and limited systemic involvement, often responding to conservative treatment. Recognising ITA as a distinct clinical entity may improve diagnosis and management strategies.
Introduction
Peritonsillar abscess (PTA) is the most common type of abscess encountered in otorhinolaryngology. In the United States, the annual incidence is reported as 30 cases per 100,000 individuals, amounting to approximately 45,000 cases per year 1. The peritonsillar space is defined as the area between the capsule of the palatine tonsil and the superior pharyngeal constrictor muscle. The accumulation of purulent material in this space characterises a peritonsillar abscess. Clinical manifestations of PTA typically include odynophagia, otalgia, trismus, and voice changes.
In contrast, an intratonsillar abscess (ITA) is defined by the formation of purulent content within the parenchyma of the palatine tonsil. The aetiology and pathogenesis of ITA remain incompletely understood. The most widely accepted mechanism involves obstruction of the crypt openings of the tonsil, leading to abscess formation within the palatine tonsil. Another proposed mechanism is bacterial seeding into the tonsil parenchyma via lymphatic or haematogenous routes 2,3.
While needle aspiration, incision, and drainage are considered standard treatment options for PTA, there is no clear consensus regarding the management of ITA 4,5. The rarity of ITA and the limited number of published studies on the subject hinder its recognition and often lead clinicians to apply PTA treatment protocols to ITA cases. However, due to the anatomical differences between these 2 types of abscesses, managing ITA in the same way as PTA may result in suboptimal outcomes.
Although PTA and ITA share some common features, they exhibit distinct clinical differences. Moreover, the initial symptoms, risk factors, natural course, treatment approaches, and clinical outcomes of ITA are not yet fully elucidated. This study aims to define these ITA-specific criteria through a comparative analysis with patients presenting with PTA.
Materials and methods
This study was approved by the Institutional Review Board for Clinical Research at our hospital and conducted in accordance with the ethical standards outlined in the Declaration of Helsinki. This single-centre retrospective study was conducted at a tertiary hospital. Patients aged 16 years and above were included, as those in the late adolescent group are referred to the ENT department for consultation, while patients under 16 years are directed to the paediatric emergency department and managed by paediatric infectious disease specialists. The study involved patients who presented to the emergency department between February 2019 and February 2025 with suspected deep neck space infections, with an age range of 16 to 76 years and a mean age of 33.2 ± 14.7 years. Since there is no specific ICD-10 code for ITA, patients were identified using the codes for PTA and acute tonsillitis. Medical records and radiological imaging of the patients were reviewed.
The primary indications for performing a CT in cases of suspected PTA or ITA include tonsillar asymmetry associated with signs of infection, uvula deviation, or persistent tonsillitis despite oral treatment, and complications such as obstruction, dysphagia and trismus. These indications are typically identified by emergency medicine specialists. If an abscess focus is detected on CT, the patient is referred to our department for consultation.
ITA was defined as either an abscess detected within the tonsillar parenchyma on CT by a radiologist or the drainage of purulent material from the intratonsillar parenchyma. PTA was defined as an abscess detected in the peritonsillar space by a radiologist or the drainage of purulent material from the peritonsillar space 6 (Fig. 1). Patients with pharyngitis, tonsillitis, parapharyngeal abscess, retropharyngeal abscess, or abscesses located in other regions of the neck were excluded from the study.
Data on age, gender, presenting symptoms, laboratory parameters (white blood cells [WBC], neutrophils, lymphocytes, large unstained cells [LUC], platelets, haemoglobin, C-reactive protein [CRP], glucose, urea, creatinine, sodium, glomerular filtration rate [GFR], procalcitonin, neutrophil-to-lymphocyte ratio [NLR], platelet-to-WBC ratio [PWR], systemic immune-inflammation index [SII]), type and outcome of the intervention performed, records of PTA or ITA recurrence, culture results, and length of hospital stay were recorded through review of the medical records. The presence of comorbid conditions was also noted in both groups. Information on pre-existing chronic diseases, such as diabetes mellitus, hypertension, asthma, coronary artery disease, etc., was extracted from patient records.
The distribution of continuous variables was assessed using the Shapiro-Wilk test. Variables with normal distribution were expressed as mean ± standard deviation, while those not normally distributed were presented as median (minimum–maximum). For comparisons between the peritonsillar and intratonsillar abscess groups, the independent samples t-test was used for normally distributed data, and the Mann-Whitney U test for non-normally distributed data. Derived indices (NLR, SII, PWR) were evaluated using the same approach. Categorical variables were presented as numbers (percentages), and differences between groups were analysed using the Chi-square test or Fisher’s exact test when the expected frequency in any cell was less than 5. All statistical tests were two-tailed, and a p value < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS Statistics software for MacOS (version 28.0, Chicago, IL, USA).
Results
A total of 367 patients were included in the study, of whom 311 (84.7%) were classified as having PTA and 56 (15.3%) as having ITA. There was no significant difference in mean age between the PTA and ITA groups (PTA: 33.7 ± 14.4 years, ITA: 30 ± 15.7 years; p = 0.105). The age range in the PTA group was 16 to 76 years, with a 95% confidence interval of 32.1 to 35.3 years, while the age range in the ITA group was 16 to 59 years, with a 95% confidence interval of 25.8 to 34.2 years. The gender distribution was also similar, with males comprising 65.3% of the PTA group and 58.9% of the ITA group (p = 0.362) (Tab. I).
Smoking was reported in 42.8% of PTA patients and 33.9% of ITA patients, with no significant difference between groups (p = 0.217). Similarly, alcohol use did not differ significantly (PTA: 9%, ITA: 10.7%; p = 0.684) (Tab. I).
The mean hospital stay was 6.1 ± 2 days in the PTA group and 5.7 ± 2.1 days in the ITA group (p = 0.082). In the PTA group, patients who underwent drainage had a significantly shorter hospital stay (6 ± 1.8 days) compared to those who did not (6.5 ± 2.4 days; p = 0.049). In the ITA group, no significant difference was observed between patients who underwent drainage (5.3 ± 1.5 days) and those who did not (5.8 ± 2.2 days; p = 0.56) (Tab. I).
Diabetes mellitus was present in 21 patients (6.8%) in the PTA group and 2 patients (3.6%) in the ITA group (Tab. V). However, HbA1c (%) measurements were available for only 13 of 21 diabetic patients in the PTA group (mean: 7.72 ± 2.14) and for one of 2 diabetic patients in the ITA group (value: 8.3). The difference between the groups was not significant (p = 0.80) (Tab. I).
When laboratory findings were analysed, significant differences were observed between the PTA and ITA groups in some inflammatory and biochemical parameters. The mean WBC count was significantly higher in the PTA group (15.39 ± 5.03) than in the ITA group (13.72 ± 4.98; p = 0.022). Similarly, neutrophil counts were significantly higher in the PTA group (12.27 ± 4.92 vs 10 ± 5.13; p = 0.002). Although lymphocyte counts were higher in the ITA group, the difference was not significant (p = 0.14). The mean LUC percentage was significantly higher in the ITA group (0.27 ± 0.27 vs 0.18 ± 0.09; p = 0.029). Haemoglobin levels were higher in the PTA group, but the difference did not reach significance (p = 0.08). Platelet counts were similar between the groups (p = 0.50) (Tab. II).
CRP levels were comparable between the groups (PTA: 108.33 ± 77.66, ITA: 109.1 ± 92.32; p = 0.94). Glucose, urea, and creatinine levels also did not differ significantly (p>0.05). However, serum sodium levels were significantly higher in the PTA group (138.63 ± 2.53) than in the ITA group (137.82 ± 2.68; p = 0.029). No significant differences were found in GFR, procalcitonin, NLR or SII. PWR was significantly higher in the ITA group (22.59 ± 8.9) than in the PTA group (20.23 ± 7.92; p = 0.046) (Tab. II).
Sore throat was common in both groups (PTA: 96.7%; ITA: 96.4%). Dysphagia was reported in 78.1% of PTA cases and 60.7% of ITA cases. Odynophagia was noted in 68.4% of PTA cases and 62.5% of ITA cases. Fever was more prevalent in the ITA group (39.2%) compared to the PTA group (19.9%). Trismus occurred in 33.4% of PTA patients and in 12.5% of ITA patients. Neck pain was reported in 6.7% of PTA cases and 3.5% of ITA cases. Lymphadenopathy was recorded in 3.2% of PTA cases and 1.7% of ITA cases. Dyspnoea and restricted neck movement were observed only in the PTA group (each in 0.9%). Otalgia was present in one PTA case (0.3%) and absent in ITA. Cough was reported in 2 PTA cases (0.6%) and in none of the ITA cases (Tab. III).
In the PTA group, the most frequently isolated organisms were Streptococcus species (93 cases) and polymicrobial growth (34 cases). Other isolates included Staphylococcus species (8), Aggregatibacter segnis (3), Eikenella corrodens (3), Serratia marcescens (2), Arcanobacterium haemolyticum (2), Pseudomonas spp. (2), Raoultella planticola (1), Klebsiella pneumoniae (1), Corynebacterium spp. (1), Enterococcus faecalis (1), Haemophilus influenzae (1), and Rothia mucilaginosa (1); in 98 cases, cultures yielded no growth. In the ITA group, Streptococcus species were isolated in 3 cases and polymicrobial growth in one case. Aggregatibacter segnis, Serratia marcescens, and Haemophilus influenzae were each isolated in one case. No growth was observed in the remaining 49 ITA patients (Tab. IV).
Comorbidities were more prevalent in the PTA group compared to the ITA group, with the PTA group showing higher percentages of conditions. In both groups, the most common conditions were diabetes mellitus, hypertension, asthma, and familial Mediterranean fever. Malignancies were found in 1% of the PTA group. On the other hand, the ITA group had a lower prevalence of comorbidities, with fewer conditions observed overall (Tab. V).
Discussion
In this study, the clinical, laboratory, and microbiological characteristics of patients with PTA and ITA were compared, and treatment-related parameters such as drainage success and length of hospital stay were evaluated. The findings demonstrate that, despite overlapping features, these 2 entities have distinct pathophysiological and clinical profiles.
PTA is commonly reported in the literature as being more prevalent among young adults (aged 20-40 years) and males 7. ITA, on the other hand, is relatively rare and has been predominantly described in children and young adults 6,8. In our study, no significant difference was observed between the PTA and ITA groups regarding age and gender 5. Although the ITA group had a lower mean age, the difference was not significant (p = 0.105).
In both patient groups, sore throat, dysphagia, and odynophagia were the most frequently reported symptoms. However, fever was more commonly observed in the ITA group (39.2% vs 19.9%), which may indicate a more prominent systemic inflammatory response. In contrast, signs of local invasion such as trismus (33.4% vs 12.5%), lymphadenopathy, and restricted neck movement were more frequent in the PTA group. The pronounced presence of trismus in PTA may be attributed to the spread of infection into the pterygomandibular space, whereas such symptoms are rarely seen in ITA 7.
Although smoking was more prevalent in the PTA group (42.8%) compared to the ITA group (33.9%), the difference was not significant. Likewise, no significant difference was found in alcohol consumption between the 2 groups. Previous studies have suggested that smoking may contribute to the development of PTA by promoting inflammation in the tonsillar crypts 9,10. However, the relationship between alcohol use and the development of PTA or ITA remains unclear.
In our study, the mean duration of hospitalisation was 6.1 days in the PTA group and 5.7 days in the ITA group. The literature reports that PTA patients are typically hospitalised for 3-7 days 5. Although data on ITA management are more limited, it has been suggested that ITA tends to follow a milder course and may resolve with medical treatment, leading to shorter hospital stays 11.
In the PTA group, patients who underwent drainage had significantly shorter hospital stays (p = 0.049). This finding supports the critical role of drainage in abscess management and its contribution to more rapid recovery 12. In the ITA group, no significant difference in hospital stay was observed between drained and non-drained patients (p = 0.56). This may be explained by the generally smaller size of ITA abscesses and their potential to resolve with antibiotic therapy alone 8.
In our study, drainage attempts were successful in 80.8% of PTA patients, but only 19.1% of ITA patients (p < 0.001) (Fig. 2). Additionally, the mean volume of drained material was significantly lower in the ITA group (1.2 mL) compared to the PTA group (4.1 mL; p = 0.048). The literature describes PTA as typically involving a well-formed abscess, in which drainage plays a key therapeutic role 13. In contrast, ITA is often characterised by smaller abscesses and is usually managed with antibiotics, since drainage procedures are frequently unsuccessful 8. This may be attributed to the small volume, high viscosity, or granulomatous nature of the ITA content 14. In clinical practice, this underscores the importance of avoiding unnecessary invasive interventions in cases of suspected ITA.
Inflammatory biomarkers were more prominent in the PTA group, with significantly elevated leukocyte and neutrophil counts, a finding that appeared to parallel the higher frequency of polymicrobial infections. In contrast, the increase in LUC observed in the ITA group was notable and may suggest a more localised inflammatory process characterised by a predominant lymphocytic response. These findings indicate that while the PTA group displayed a more pronounced neutrophilic inflammatory profile, the ITA group was characterised by alternative patterns of inflammation. Similar observations regarding the diagnostic and prognostic value of inflammatory indices in deep neck infections have been reported by Fiorella et al., highlighting the utility of such markers in clinical decision-making 15. Although procalcitonin levels remained low and showed no significant difference between groups, this may be attributed to the generally favourable clinical course observed in both groups.
No significant difference in HbA1c levels was found between the PTA and ITA groups (p = 0.80). While diabetes has been previously identified as a notable risk factor for recurrent PTA, data supporting a relationship between diabetes and ITA remain limited 1. As HbA1c measurements were available for only a subset of patients in our study, further research with larger sample sizes is warranted to explore this potential association.
Microbiological analysis revealed that PTA patients more frequently harboured pathogens such as Streptococcus species (especially Streptococcus pyogenes), as well as Staphylococcus aureus, Klebsiella pneumoniae, and Pseudomonas aeruginosa. In contrast, bacterial growth in the ITA group was limited to a small number of cases, with only a few organisms identified. Polymicrobial infections were notably prevalent only in the PTA group, whereas such occurrences were rare in ITA. These results suggest that PTA tends to present as a more complex and extensive infectious process, while ITA may represent a more localised condition primarily associated with inflammatory changes 16.
In our study, comorbidities, particularly chronic diseases such as diabetes mellitus and hypertension, were observed more frequently in patients with peritonsillar abscess compared to those with intratonsillar abscess. Malignancies and other severe chronic conditions were almost exclusively present in the PTA group. While comorbid conditions such as diabetes and hypertension appeared more frequently in the PTA group, the difference was not significant, indicating that chronic diseases may play a limited role in differentiating between PTA and ITA patients 5.
The study had several limitations. First, it was a single-centre retrospective design, which limits the generalisability of the findings to broader populations and other clinical settings. Retrospective designs also introduce potential biases related to data collection. Second, patients under 16 years of age were not included, as they are typically managed by paediatric infectious disease departments, meaning the conclusions may not apply to paediatric populations. Third, HbA1c measurements were only available for a subset of patients, which limited the ability to explore the potential association between diabetes and ITA comprehensively. This is an area where further research with larger sample sizes is needed. Another important limitation of the study was related to the microbiological analysis. A substantial proportion of ITA cases (85.7%) were either not drained or had unsuccessful drainage, which significantly limited the ability to obtain adequate purulent material for culture.
Conclusions
This study demonstrates that PTA and ITA exhibit distinct clinical courses and management characteristics. Drainage was identified as a crucial therapeutic intervention in PTA, which typically involved larger abscess volumes. In contrast, ITA was more often associated with smaller abscesses and could generally be managed without drainage. Our findings emphasise that ITA should be recognised as a separate clinical entity from PTA. Future prospective studies with larger sample sizes are needed to further elucidate these differences. Additionally, the prognostic value of laboratory parameters in ITA should be further investigated.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This study was not funded by any specific grants from public, commercial, or non-profit funding agencies.
Author contributions
KSB, AO, BC: conceptualization; KSB, AO, SS, BC, TSDB: data curation; KSB, FG, MAB, SS: formal analysis; KSB, TSDB, FG: writing – original draft; KSB, TSDB, MAB: writing – review and editing.
Ethical consideration
The study received approval from the Medical Research Scientific and Ethical Review Board of Ankara Bilkent City Hospital (Protocol No: 1-25-1146). All procedures were carried out in compliance with ethical standards and adhered to the principles outlined in the World Medical Association Declaration of Helsinki.
History
Received: May 2, 2025
Accepted: July 30, 2025
Figures and tables
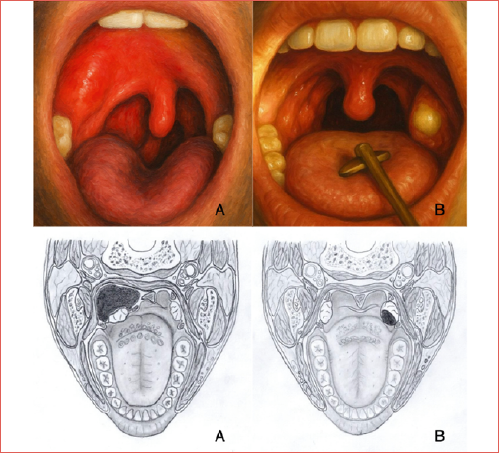
Figure 1. Contrast-enhanced neck computed tomography shows (A) an intratonsillar abscess in the left tonsil (arrow) and (B) a peritonsillar abscess in the left peritonsillar space with medial displacement of the tonsil (arrow).
Figure 2. Patient flow and outcomes of drainage attempts in the PTA and ITA groups.
| Peritonsillar group | Intratonsillar abscess | p value | |||
|---|---|---|---|---|---|
| (n = 311) | (n = 56) | ||||
| n (%) | mean ± SD | n (%) | mean ± SD | ||
| Age, y | 33.7 ± 14.4 | 30 ± 15.7 | 0.105 | ||
| Gender | |||||
| Female | 108 (34.7) | - | 23 (41.1) | - | 0.362 |
| Male | 203 (65.3) | - | 33 (58.9) | - | |
| Smoking status | |||||
| Yes | 133 (42.8) | - | 19 (33.9) | - | 0.217 |
| No | 178 (57.2) | - | 37 (66.1) | - | |
| Alcohol status | |||||
| Yes | 28(9) | - | 6 (10.7) | - | 0.684 |
| No | 283(91) | - | 50 (89.3) | - | |
| Length of stay, day | - | 6.1 ± 2 | - | 5.79 ± 2.14 | 0.082 |
| Result of drainage attempt | |||||
| Successful | 251 (85.1) | - | 8 (19.1) | - | < 0.001 |
| Unsuccessful | 44 (14.9) | - | 34 (80.9) | - | |
| HbA1c, % | 13 (4.1) | 7.72 ± 2.14 | 1(1.7) | 8.3 | 0.80 |
| Amount of drainage, mL | - | 4.11 ± 4.1 | 1.25 ± 0.7 | 0.048 | |
| Peritonsillar abscess (n = 311) | Intratonsillar abscess (n = 56) | p value | |
|---|---|---|---|
| (n = 56) | mean ± SD | ||
| WBC, 109/L | 15.39 ± 5.03 | 13.72 ± 4.98 | 0.022 |
| Neutrophils, 109/L | 12.27 ± 4.92 | 10 ± 5.13 | 0.002 |
| Lymphocytes, 109/L | 1.92 ± 0.76 | 2.29 ± 1.86 | 0.14 |
| LUC, 109/L | 0.18 ± 0.09 | 0.27 ± 0.27 | 0.029 |
| Haemoglobin, g/dL | 14.24 ± 1.73 | 13.81 ± 1.74 | 0.08 |
| Platelet, 109/L | 287.42 ± 84.81 | 279.32 ± 80.57 | 0.50 |
| CRP, mg/L | 108.33 ± 77.66 | 109.1 ± 92.32 | 0.94 |
| Glucose, mg/dL | 98.19 ± 29.94 | 97.7 ± 23.59 | 0.90 |
| Urea, mg/dL | 28.64 ± 9.65 | 27.98 ± 17.68 | 0.68 |
| Creatinine, mg/dL | 0.77 ± 0.18 | 0.77 ± 0.24 | 0.79 |
| Sodium, mmol/L | 138.63 ± 2.53 | 137.82 ± 2.68 | 0.029 |
| GFR, mL/min/1.73 m2 | 111.05 ± 16.12 | 108.88 ± 19.11 | 0.36 |
| Procalcitonin, ng/mL | 0.11 ± 0.22 | 0.16 ± 0.33 | 0.24 |
| NLR | 7.80 ± 6.37 | 6.76 ± 9.18 | 0.29 |
| PWR | 20.23 ± 7.92 | 22.59 ± 8.9 | 0.046 |
| SII | 2263.85 ± 2690.88 | 1881.85 ± 2892.63 | 0.33 |
| WBC: white blood cell; LUC: large unstained cells; CRP: C-reactive protein; GFR: glomerular filtration rate; NLR: neutrophil-to-lymphocyte ratio; PWR: platelet-to-WBC ratio; SII: systemic immune-inflammation index. | |||
| Overall, n = 367 | PTA, n = 311 | ITA, n = 56 | |
|---|---|---|---|
| n, % | n, % | n, % | |
| Neck pain | 23 (6.2) | 21 (6.7) | 2 (3.5) |
| Sore throat | 355 (96.7) | 301 (96.7) | 54 (96.4) |
| Odynophagia | 248 (67.5) | 213 (68.4) | 35 (62.5) |
| Dysphagia | 277 (75.4) | 243 (78.1) | 34 (60.7) |
| Fever | 84 (22.8) | 62 (19.9) | 22 (39.2) |
| Dyspnoea | 3 (0.8) | 3 (0.9) | 0 (0) |
| Trismus | 111 (30.2) | 104 (33.4) | 7 (12.5) |
| Lymphadenopathy | 11 (2.9) | 10 (3.2) | 1 (1.7) |
| Restriction of cervical range of motion | 3 (0.8) | 3 (0.9) | 0 (0) |
| Otalgia | 1 (0.3) | 1 (0.3) | 0 (0) |
| Cough | 2 (0.5) | 2 (0.6) | 0 (0) |
| PTA: peritonsillar abscess; ITA: intratonsillar abscess. | |||
| PTA, n = 311 | ITA, n = 56 | |
|---|---|---|
| n, % | n, % | |
| Polymicrobial | 34 (10.9%) | 1 (1.8%) |
| Aggregatibacter segnis | 3 (1%) | 1 (1.8%) |
| Arcanobacterium haemolyticum | 2 (0.6%) | 0 (0%) |
| Eikenella corrodens | 3 (1%) | 0 (0%) |
| Raoultella planticola | 1 (0.3%) | 0 (0%) |
| Klebsiella pneumoniae | 1 (0.3%) | 0 (0%) |
| Staphylococcus spp. | 8 (2.6%) | 0 (0%) |
| Serratia marcescens | 2 (0.6%) | 1 (1.8%) |
| Corynebacterium spp. | 1 (0.3%) | 0 (0%) |
| Streptococcus spp. | 93 (29.9%) | 3 (5.4%) |
| Enterococcus faecalis | 1 (0.3%) | 0 (0%) |
| Pseudomonas spp. | 2 (0.6%) | 0 (0%) |
| Haemophilus influenzae | 1 (0.3%) | 1 (1.8%) |
| Rothia mucilaginosa | 1 (0.3%) | 0 (0%) |
| No bacterial growth | 98 (31.5%) | 1 (1.8%) |
| Undrained and unsuccessful drainages | 60 (19.3%) | 48 (85.7%) |
| PTA: peritonsillar abscess; ITA: intratonsillar abscess. | ||
| PTA, n = 311 | ITA, n = 56 | |
|---|---|---|
| n, % | n, % | |
| Diabetes mellitus | 21 (6.8%) | 2 (3.6%) |
| Hypertension | 10 (3.2%) | 2 (3.6%) |
| Asthma | 7 (2.3%) | 2 (3.6%) |
| Coronary artery disease | 5 (1.6%) | 0 (0%) |
| Hyperlipidaemia | 4 (1.3%) | 0 (0%) |
| Benign prostatic hyperplasia | 2 (0.6%) | 0 (0%) |
| Hepatitis B infection | 2 (0.6%) | 0 (0%) |
| Chronic obstructive pulmonary disease | 1 (0.3%) | 0 (0%) |
| Alzheimer’s disease | 1 (0.3%) | 0 (0%) |
| Migraine | 1 (0.3%) | 0 (0%) |
| Panic disorder | 1 (0.3%) | 0 (0%) |
| Epilepsy | 1 (0.3%) | 0 (0%) |
| Depression | 2 (0.6%) | 0 (0%) |
| Hypothyroidism | 3 (1%) | 0 (0%) |
| Hyperthyroidism | 1 (0.3%) | 0 (0%) |
| Familial Mediterranean fever | 3 (1%) | 2 (3.6%) |
| Multiple sclerosis | 0 (0%) | 1 (1.8%) |
| Parkinson’s disease | 1 (0.3%) | 0 (0.0%) |
| Malignancies (bladder, colon, tongue cancer) | 3 (1%) | 0 (0.0%) |
| PTA: peritonsillar abscess; ITA: intratonsillar abscess. | ||
References
- Johnson R, Stewart M, Wright C. An evidence-based review of the treatment of peritonsillar abscess. Otolaryngol Head Neck Surg. 2003;128:332-343. doi:https://doi.org/10.1067/mhn.2003.93
- Hur K, Zhou S, Kysh L. Adjunct steroids in the treatment of peritonsillar abscess: a systematic review. Laryngoscope. 2018;128:72-77. doi:https://doi.org/10.1002/LARY.26672
- Blair A, Booth R, Baugh R. A unifying theory of tonsillitis, intratonsillar abscess and peritonsillar abscess. Am J Otolaryngol. 2015;36:517-520. doi:https://doi.org/10.1016/J.AMJOTO.2015.03.002
- Chang B, Thamboo A, Burton M. Needle aspiration versus incision and drainage for the treatment of peritonsillar abscess. Cochrane Database Syst Rev. 2016;12. doi:https://doi.org/10.1002/14651858.CD006287.PUB4
- Herzon F. Harris P. Mosher Award thesis. Peritonsillar abscess: incidence, current management practices, and a proposal for treatment guidelines. Laryngoscope. 1995;105:1-17. doi:https://doi.org/10.1288/00005537-199508002-00001
- Ali S, Kovatch K, Smith J. Predictors of intratonsillar versus peritonsillar abscess: a case-control series. Laryngoscope. 2019;129:1354-1359. doi:https://doi.org/10.1002/lary.27615
- Klug T. Peritonsillar abscess: clinical aspects of microbiology, risk factors, and the association with parapharyngeal abscess. Dan Med J. 2017;64.
- Giurintano J, Kortebein S, Sebelik M. Intratonsillar abscess: a not-so-rare clinical entity. Int J Pediatr Otorhinolaryngol. Published online 2019. doi:https://doi.org/10.1016/j.ijporl.2018.12.039
- Klug T, Rusan M, Clemmensen K. Smoking promotes peritonsillar abscess. Eur Arch Otorhinolaryngol. 2013;270:3163-3167. doi:https://doi.org/10.1007/s00405-013-2474-4
- Clark C, Santarelli A, Merrill S. Analysis of smoking behavior in patients with peritonsillar abscess: a rural community hospital’s experience. Cureus. 2022;14. doi:https://doi.org/10.7759/cureus.23300
- Mitchelmore I, Prior A, Montgomery P. Microbiological features and pathogenesis of peritonsillar abscesses. Eur J Clin Microbiol Infect Dis. 1995;14:870-877. doi:https://doi.org/10.1007/BF01691493
- Passy V. Pathogenesis of peritonsillar abscess. Laryngoscope. 1994;104:185-190. doi:https://doi.org/10.1288/00005537-199402000-00011
- Maharaj D, Rajah V, Hemsley S. Management of peritonsillar abscess. J Laryngol Otol. 1991;105:743-745. doi:https://doi.org/10.1017/S0022215100117189
- Ahmed Ali S, Kovatch K, Smith J. Predictors of intratonsillar abscess versus peritonsillar abscess in the pediatric patient. Int J Pediatr Otorhinolaryngol. 2018;114:143-146. doi:https://doi.org/10.1016/j.ijporl.2018.08.042
- Fiorella M, Greco P, Madami L. New laboratory predictive tools in deep neck space infections. Acta Otorhinolaryngol Ital. 2020;40:332-337. doi:https://doi.org/10.14639/0392-100X-N0790
- Brook I. Microbiology and management of peritonsillar, retropharyngeal, and parapharyngeal abscess. J Oral Maxillofac Surg. 2004;62:1545-1550. doi:https://doi.org/10.1016/j.joms.2003.12.043
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 480 times
- PDF downloaded - 82 times