Laryngology
Vol. 46: Issue 3 - June 2026
The effect of aryepiglottic fold release as an adjuvant step in surgery for Type I laryngomalacia
Summary
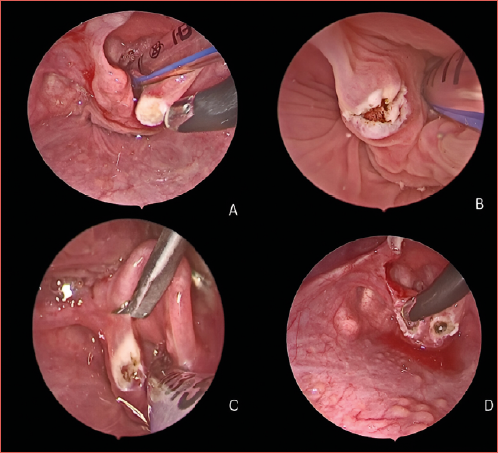
Cover Image
Objective. This study aims to evaluate the efficacy of unilateral aryepiglottic fold release as an adjunctive surgical step in the management of Type I laryngomalacia.
Methods. This study was prospectively conducted on a sample of paediatric patients with laryngomalacia. Our patients were randomly divided into Group A (study group, n = 25), undergoing adjuvant aryepiglottic fold release (AEFR), and Group B (control group, n = 25), who did not undergo adjuvant AEFR. Demographic data, clinical features, and outcome measures were compared between groups.
Results. A highly significant difference was observed in the time to resolution of postoperative stridor, with the study group demonstrating markedly earlier symptom resolution compared to the control group. Furthermore, the percentage change in oxygen saturation in both states was also significantly greater in the study group, reflecting a highly significant intergroup difference. Additionally, the incidence of perioperative respiratory adverse events (PRAEs) was significantly lower in the study group than in the control group.
Conclusions. Unilateral AEFR, as an adjunctive procedure, marks a significant advancement in management of Type I laryngomalacia. It offers targeted improvement in oxygen saturation levels during both wakefulness and sleep. Furthermore, the technique has been shown to decrease the incidence of PRAEs, delivering significant clinical and operational benefits.
Introduction
Laryngomalacia is the most common congenital laryngeal disorder in infants. It often presents with stridor and may be accompanied by respiratory distress, apnoea episodes, cyanosis, choking, microaspiration, and poor weight gain or failure to thrive 1,2. It is frequently a self-limiting condition that tends to improve over time without intervention. However, around 10-20% of cases necessitate surgical management due to progressive symptoms unresponsive to conservative measures or development of serious complications, including severe stridor, cyanotic episodes, failure to thrive, pulmonary hypertension, or the onset of pectus excavatum 3. The exact cause of laryngomalacia remains uncertain, but proposed theories suggest it may involve insufficient rigidity of the laryngeal cartilages, inflammation due to gastro-oesophageal reflux disease (GERD), or impaired neuromuscular control of the larynx 4.
Laryngomalacia is categorised based on its laryngoscopic appearance, with the widely used Olney classification identifying 3 Types: Type I is characterised by mucosal prolapse over the arytenoid cartilages, Type II involves shortened aryepiglottic folds, and Type III is defined by posterior displacement of the epiglottis. In many cases, a combination of these anatomical patterns may be present 5.
Supraglottoplasty is the standard surgical treatment for severe laryngomalacia. The procedure can be performed using microlaryngeal cold instruments 6, CO2 laser 7, or coblation techniques 8. Outcomes achieved with these different methods are comparable and demonstrate similar effectiveness 9. Perioperative respiratory adverse events (PRAEs) requiring intensive care unit (ICU)-level support can occur following supraglottoplasty. Given the substantial costs and risks associated with ICU admission, efforts should be directed toward identifying strategies to reduce unnecessary ICU utilisation 10.
Seid et al. described dividing the aryepiglottic folds to elongate the laryngeal inlet in the anteroposterior axis as an independent procedure for managing laryngomalacia 11. This study aims to evaluate the efficacy of unilateral AEFR as an adjunctive surgical step in the management of Type I laryngomalacia.
Materials and methods
Study design
This prospective case-control study was conducted over a 42-month period, from June 2021 to December 2024, at the Departments of Otorhinolaryngology – Head and Neck Surgery of Kafrelsheikh and Mansoura University Hospitals. The study enrolled 50 patients who were diagnosed with Type I laryngomalacia.
The present clinical research was carried out in compliance with the currently approved Institutional Review Board (IRB) protocol, as well as the applicable policies, regulations, and ethical standards of Kafrelsheikh University. The investigator provided a detailed explanation to the guardians regarding the study’s significance, objectives, and participants’ rights. Written informed consent was obtained from all guardians before initiation of the study.
All consecutive patients with laryngomalacia who came to the Otorhinolaryngology outpatient clinic or the Emergency Department seeking advice, or who were referred from children’s hospitals, were eligible for inclusion in the study. The study included 50 patients diagnosed with Type I laryngomalacia who had no history of previous supraglottoplasty and were deemed suitable candidates for surgical intervention. Patients were excluded if they had undergone prior supraglottoplasty or were considered unfit for surgery.
This study was prospectively conducted on a sample of paediatric laryngomalacia patients. Our patients were randomly divided into Group A (study group, n = 25), undergoing adjuvant aryepiglottic fold release, and Group B (control group, n = 25), who did not undergo adjuvant aryepiglottic fold release. Randomisation was done by using the block randomisation method.
Preoperative evaluation
The clinical assessment included a detailed history focusing on the onset of stridor, sleep-related symptoms, feeding challenges, cyanotic episodes, and growth issues. Feeding and swallowing difficulties, such as choking, coughing, or regurgitation during meals, were noted.
Vital signs were recorded, including oxygen saturation while awake and sleeping. Pre- and postoperative lowest oxygen saturation levels were recorded using an overnight pulse oximeter. Signs of respiratory distress were observed, such as flaring nostrils, and various types of retractions (suprasternal, intercostal, subcostal), as well as pectus excavatum. A paediatric consultant ruled out concurrent cardiac issues or congenital anomalies. Laryngomalacia was classified according to the Thompson severity score into 3 grades: mild, moderate, and severe 1.
Each patient underwent an awake endoscopic evaluation using a lubricated flexible fibreoptic laryngoscope (FFL) with a high-definition camera and monitor (Karl Storz H3-Z TH100). A 4 mm endoscope was preferred for optimal visualisation. The scope was inserted above the inferior turbinate to minimise endonasal trauma. The examination included a thorough evaluation of the nasal passages, nasopharynx, tongue base, supraglottic larynx, and vocal folds, along with an initial assessment of the subglottic region. Laryngomalacia was classified into Types I, II, and III based on Olney et al. 5. We used the Olney classification to define Type I laryngomalacia patients, which were included in our study. Any concurrent airway abnormalities were documented at this stage.
Flexible endoscopic evaluation of swallowing (FEES) was conducted for each case, following the same awake endoscopic procedure. Various food consistencies were used, including thin liquids, yogurt, pureed, and solid food when appropriate for the child’s age. For infants under 6 months, formula milk was used. Aspiration, penetration, or premature spillage with each food type was recorded. The Penetration-Aspiration Scale 3 was used to assess aspiration severity. FEES examinations were performed before surgery and one month later.
In cases presenting with moderate to severe symptoms, additional diagnostic evaluations were performed to guide clinical management. These assessments included echocardiography to identify any associated cardiac anomalies, pulmonary hypertension, or right-sided heart failure; overnight pulse oximetry (Level 4 sleep study) to objectively measure the severity of sleep-related symptoms; and arterial blood gas analysis to detect signs of chronic hypoxia or hypercapnia.
Surgical technique
The procedure typically began with a dynamic fibreoptic examination of the entire airway while the infant maintained spontaneous respiration under sevoflurane inhalational anaesthesia. A fibreoptic endoscope was routinely passed through the vocal cords to evaluate any static or dynamic abnormalities in the distal airway. Following this assessment, endotracheal intubation was performed to initiate surgical intervention.
Coblation was carried out using the Coblator 2 Arthrocare system (Austin, Texas, USA), employing either a Procise Mini Laryngeal Wand (MLW) or a Procise Laryngeal Wand (LW), depending on the surgical site (Cover figure). Traditional laryngeal suspension techniques were not utilised. Instead, exposure of the supraglottic larynx was achieved using a Macintosh laryngoscope, held in position by an assistant to provide adequate tension in the targeted tissue. The surgeon operated a 30° endoscope with the left hand and the coblation wand with the right, while the entire surgical team viewed the procedure in real-time on a monitor.
In Group A (study group), the laryngeal wand (LW) was selected to provide a more potent effect on cartilage. Cuneiform cartilage was ablated, trying hard to preserve the surrounding aryepiglottic fold mucosa, especially anteriorly, to avoid its excessive shortening and ensuing airway stenosis. Redundant arytenoid mucosa was ablated whenever needed. We used scissors to cut the aryepiglottic fold very close to the edge of the epiglottis and down to the ventricular fold to minimise mucosal loss.
In Group B (control group), the LW was selected to provide a more potent effect on cartilage. Cuneiform cartilage was ablated, trying hard to preserve the surrounding aryepiglottic fold mucosa, especially anteriorly, to avoid shortening and stenosis. Redundant arytenoid mucosa was ablated whenever needed without aryepiglottic fold release.
Postoperative management
All children were successfully extubated immediately after the procedure, with no postoperative complications. An early postoperative evaluation was conducted to assess stridor, cyanosis, and minimum oxygen saturation levels. Patients were observed overnight in the paediatric ICU. Oral feeding was resumed 6 hours after surgery, with particular attention given to assessing any signs of choking. Pain was controlled using paracetamol, and one-week course of antibiotics was administered. Acid suppression therapy was provided following the International Pediatric Otorhinolaryngology Group (IPOG) guidelines 13. Follow-up awake endoscopy was performed 2-3 weeks postoperatively. Comprehensive clinical assessments were conducted at one and 3 months after surgery to evaluate the persistence or resolution of symptoms.
Evaluation of outcomes
After surgery, the operation-specific success rate (OSSR) was defined as the complete resolution or significant improvement of initial symptoms, eliminating the need for further medical intervention. Conversely, failure was characterised by inadequate symptom improvement necessitating additional measures, such as revision surgery, extended use of non-invasive ventilation or oxygen therapy, or tracheotomy 14.
The PRAEs were documented in both groups. They were defined as any of the following events or requirements within 24 hours from surgery: 1) failure to extubate, 2) reintubation, 3) need for positive pressure ventilation, 4) need for more than one dose of racemic epinephrine, or 5) need for more than 4 litres of oxygen via nasal cannula 10.
Both groups were compared regarding demographic and clinical data, as well as the outcomes of treatment.
Statistical evaluation was conducted using the Statistical Package for the Social Sciences (SPSS) software, version 28. Categorical data were represented as absolute frequencies and analysed using the chi-square test, with the Fisher exact test applied when appropriate. The Shapiro-Wilk test was employed to confirm the suitability of parametric test assumptions. Quantitative data were summarised either as means with standard deviations or medians with interquartile ranges, depending on the data distribution.
Comparisons between 2 groups for quantitative data were made using either an independent sample t-test (for data with a normal distribution) or the Mann-Whitney test (for non-normally distributed data). For within-group comparisons of variables over 2 time points, binary categorical data were analysed with the McNemar test, and normally distributed continuous data were assessed using a paired sample t-test. The percent change in outcome parameters was calculated using the formula: [(postoperative value − preoperative value)/preoperative value] ×100. The level for statistical significance was established at p < 0.05, with a value of p ≤ 0.001 indicating a highly significant difference.
Results
Our study included 31 males (62%) and 19 females (38%), with a median age of 18 months at the time of surgery. There were no significant differences between groups regarding age or gender. Comorbidities were documented in 34% of the patients in our study. The most common associated problems were neurological (7 cases) and synchronous airway anomalies (7 cases), followed by cardiac abnormalities (4 cases). No significant intergroup differences were found concerning comorbidities, presenting symptoms, or clinical signs (Tab. I).
All patients experienced preoperative stridor. Postoperatively, there was no significant difference in stridor occurrence between the groups. However, within each group, there was a highly significant reduction in the frequency of patients presenting with stridor after surgery (p < 0.001) (Tab. II).
Regarding pre- and postoperative outcomes, there were no significant differences between the groups in rates of failure to thrive (FTT), choking, or cyanosis. However, within each group, there was a significant reduction in FTT postoperatively compared to preoperative levels. While choking and cyanosis frequencies also decreased postoperatively, these reductions were not significant (Tab. II).
Operative time did not significantly differ between the groups (Tab. III). However, a highly significant difference was noted in the time to resolution of postoperative stridor, with the study group achieving symptom resolution significantly earlier (Tab. IV).
Preoperatively, oxygen saturation during sleep did not differ significantly between groups, but a significant difference was noted in awake oxygen saturation, favouring the study group. Postoperatively, oxygen saturation during both sleep and awake states was significantly higher in the study group compared to the control group. Within each group, postoperative oxygen saturation showed a highly significant increase compared to preoperative levels, both during sleep and while awake (Tab. V).
There was a highly significant difference between groups regarding the percent change in oxygen saturation during both sleep and awake states (significantly higher in the study group) (Tab. VI).
The overall success rate was 96% in the study group and 88% in the control group, although this difference was not significant. However, a significant reduction in the incidence of PRAEs was observed in the study group compared to the control group (Tab. VII).
Discussion
Laryngomalacia is characterised by inspiratory collapse of the flaccid supraglottic structures, leading to varying degrees of airway obstruction 15. The primary symptom of laryngomalacia is typically “noisy breathing”, although many patients also experience feeding difficulties such as choking, regurgitation, and FTT. Due to airway obstruction, infants with laryngomalacia may struggle to coordinate the suck-swallow-breathe sequence required for effective feeding 16. Most infants with laryngomalacia present with mild symptoms that generally resolve spontaneously by 12 to 24 months of age. However, not all cases follow such a benign course 2. Approximately 10% of cases require surgical intervention, primarily for complications such as apnoea or significant respiratory distress. The second most common indication for surgery is poor weight gain 17,18.
Currently, there is no universally accepted or validated classification system for laryngomalacia. Several types and classification schemes have been described in the literature, with varying levels of adoption 1,2,4,5. In 1999, Olney et al. introduced a classification that remains one of the most widely used based on variations in supraglottic anatomy 5. In our study, we used the Olney’s classification to define Type I laryngomalacia. This system was chosen for its simplicity, ease of application, widespread use in clinical practice, and its correlation with the surgical procedure if the patient requires a supraglottoplasty.
Laryngomalacia has also been classified by severity into 3 grades – mild, moderate, and severe – using the Thompson severity score 1. This severity-based classification aids clinicians in tailoring management strategies based on symptom severity and associated risks. In our study, 28 patients (56%) were categorised as having moderate laryngomalacia. There was no significant difference between groups studied regarding the grade of laryngomalacia.
Among the 50 patients in our study, 31 were males (62%) and 19 females (38%), with a median age of 18 months at the time of surgery. Similarly, Reinhard et al. 14 conducted a study involving 79 patients, comprising 44 males (55.7%) and 35 females (44.3%), with an average age of 21.9 months at the time of laser supraglottoplasty (LSGP) for Type I laryngomalacia. Another study reported a notable male predominance among children diagnosed with laryngomalacia, with males accounting for 71.1% of participants, resulting in a male-to-female ratio of 2.5:1. The age of surgically treated children varied by type of laryngomalacia, with a mean age of 51.6 weeks for Type I cases 19.
In our study, comorbidities were observed in 34% of patients. The most common associated anomalies were neurological conditions (7 cases) and synchronous airway anomalies (7 cases), followed by cardiac problems (4 cases). Children with laryngomalacia frequently have synchronous airway lesions (SALs), with reported incidence rates ranging from 7.7% to 51.7% 20,21. Bredun et al. identified SALs in 15.1% of children with laryngomalacia, with common associated anomalies including laryngotracheo-oesophageal cleft (61.1%), tracheomalacia/tracheobronchomalacia (16.7%), and trachea-oesophageal fistula (5.6%) 19. Similarly, Mancuso et al. found that SALs occurred in 18.9% of cases, emphasising their prevalence 22. Given the clinical significance of SALs, endoscopic evaluations for laryngomalacia must include a thorough assessment of the lower airways to identify and manage these associated conditions 23. Reinhard et al. 14 reported comorbidities in 55.7% of patients, including neurological disorders (16.5%), SALs (32.9%), prematurity (22.8%), and severe GERD (41.8%).
While laryngomalacia is often characterised by distinctive stridor, diagnosis based solely on an infant’s breathing sounds is not entirely reliable 24. A definitive diagnosis requires direct visualisation of the larynx. In severe cases, endoscopic examination under general anaesthesia is crucial for confirming the diagnosis and ruling out associated respiratory tract anomalies. Mancuso et al. found such anomalies in 18.9% of cases 22.
Advancements in surgical techniques over recent decades have established supraglottoplasty as the preferred treatment for laryngomalacia. The primary goal of this procedure is to remove or reshape redundant supraglottic tissue, stabilising the airway and preventing inspiratory collapse and obstruction 14. LSGP has become increasingly favoured for its superior haemostatic capabilities; however, in the majority of cases, effective bleeding control can still be achieved using topical vasoconstrictors such as adrenaline or oxymetazoline 14,25. The CO2 laser, while effective, has limitations, including high costs, lengthy setup times, risk of airway fires, and potential thermal damage to underlying tissues, which may result in pain, oedema, scarring, and dysphagia 25.
Cutting the aryepiglottic folds provides immediate and practical results, allowing seamless extubation during the procedure 26. Studies comparing surgical instruments for laryngomalacia treatment have not identified any specific tool as having a higher risk of supraglottoplasty failure 27. Historically, cold steel instruments have been the most commonly used technique, preferred by 73% of surgeons performing supraglottoplasty. The CO2 laser, favoured by 14%, is the second most common tool, with both methods achieving comparable success rates 28. Coblation offers several advantages over other surgical techniques, including reduced postoperative pain, minimal bleeding, and faster healing. It has become increasingly popular in airway surgery for procedures such as tonsillectomy and uvulopalatoplasty and is now being widely adopted for laryngeal surgeries, including the treatment of respiratory papillomatosis 29,30. Compared to CO2 laser, coblation significantly reduces the risk of airway fire and thermal injury, making it a safer option for performing supraglottoplasty while maintaining safe endotracheal intubation.
The high-energy plasma generated by coblation enables rapid tissue removal with excellent haemostasis, minimising bleeding. Additionally, its unique ablative properties, combined with tactile feedback, allow for precise control over surgical depth, offering a significant advantage over CO2 lasers. Coblation also outperforms traditional cold steel techniques in achieving effective tissue ablation while maintaining superior hemostasis 31. In a study by Ching et al., coblation was utilised for unilateral aryepiglottic fold division and mucosal ablation over the arytenoid cartilage, preserving mucosal flaps. This technique achieved successful outcomes through lateralisation of the medial flap, underscoring coblation versatility and precision in managing laryngeal conditions 31.
The primary symptom of laryngomalacia is stridor, even if its loudness does not always correlate with the severity of the condition. Some infants with severe laryngomalacia may exhibit minimal or no significant stridor 32. In our study, postoperative stridor frequency significantly decreased in both groups. While all patients experienced stridor preoperatively, only 4 (8%) continued to have stridor after surgery. The success rate was 96% in the study group and 88% in the control group, with no significant difference in outcomes between groups. However, there was a highly significant difference in the time to stridor resolution, which occurred earlier in the study group.
Regarding oxygen saturation, supraglottic tissue prolapse is known to persist during both wakefulness and sleep, with symptoms often worsening during sleep due to immature neurological mechanisms regulating airway patency and breathing 33. Assessing oxygen saturation in both states is therefore crucial. In this study, improvements in oxygen saturation during wakefulness and sleep were observed in both groups, consistent with findings by Mase et al., which demonstrated improvements in polysomnographic oxygen nadir values 33. Postoperatively, there was a significant improvement in oxygen saturation during both wakefulness and sleep in the study group compared to the control group. Additionally, the percent change in oxygen saturation during sleep and wakefulness was significantly higher in the study group. Within each group, there was also a significant reduction in the frequency of patients with FTT postoperatively compared to preoperative levels.
El-Sobki et al.34 similarly reported a significant reduction in stridor frequency among Type I laryngomalacia patients after surgery. While all patients exhibited stridor preoperatively, only 3 (10.7%) continued to have stridor postoperatively. Choking incidents also decreased significantly, from 46.4% preoperatively to 25% postoperatively (p = 0.031). Across all types of laryngomalacia, patients demonstrated notable postoperative improvements in oxygen saturation during both sleep and wakefulness compared to preoperative measurements 34.
Reinhard et al. 14 reported that the most commonly observed symptoms and indications for supraglottoplasty were stridor (93.7%), chest retractions (69.6%), feeding difficulties or failure to thrive (43%), and episodes of desaturation, cyanosis, or apnoea (27.8%). The success rate of the procedure varied based on the type of laryngomalacia, with Type I achieving a 90.5% success rate. Improvement in feeding symptoms after supraglottoplasty is likely due to the resolution of airway obstruction, which allows better coordination of breathing, sucking, and swallowing mechanisms 35. In this study, all patients were monitored postoperatively in the paediatric ICU. However, PRAEs requiring ICU intervention occurred in only 2 cases within the study group. A significant difference was noted between groups, with a significantly lower incidence of PRAEs in the study group.
A recent survey of Paediatric Otolaryngologists found that 53% routinely admit patients to a paediatric ICU after surgery, and 13% leave patients intubated postoperatively 36. However, PRAEs remain a potential complication following supraglottoplasty. Strategies to minimise PRAEs include thorough preoperative assessment, appropriate selection of surgical and anaesthesia techniques, and vigilant postoperative monitoring, particularly for patients with additional risk factors. In the study by Zheng et al., PRAEs requiring ICU-level intervention were observed in 41% of cases 37.
In a 2009 study by Schroeder et al., 63% of patients required postoperative airway support after supraglottoplasty, with one-third needing postoperative intubation 38. More recent studies, however, report lower rates of ICU-level interventions, ranging from 4.5% to 28.5%, suggesting that a more selective approach to ICU admissions may be warranted 39-42. Children undergoing airway-related surgeries are often at increased risk of PRAEs due to chronic airway inflammation and bronchial hypersensitivity. Surgical manipulation of the airway can exacerbate this risk by triggering laryngeal reflex responses, further complicating postoperative outcomes 43.
In summary, the study group demonstrated significantly better outcomes in terms of earlier stridor resolution, improved oxygen saturation, and lower rates of perioperative respiratory adverse events. To the best of our knowledge, this is the first study evaluating the impact of unilateral AEFR as an adjunctive step in managing Type I laryngomalacia. The prospective case-control design of this study is one of its significant strengths. Nonetheless, this study has certain limitations. It does not compare the outcomes of unilateral AEFR with other techniques, such as cold steel or CO2 laser. Additionally, the impact of specific comorbidities could not be thoroughly analysed due to the limited number of patients with each condition. Future research involving larger patient cohorts and comparative studies is strongly recommended to validate these findings and comprehensively assess potential long-term benefits.
Conclusions
Unilateral AEFR, as an adjunctive procedure, marks a significant advancement in management of Type 1 laryngomalacia. It offers targeted improvement in oxygen saturation levels during both wakefulness and sleep. Our findings underscore its effectiveness in alleviating symptoms such as stridor, feeding difficulties, and compromised oxygen saturation, with a low incidence of complications. The precision and safety of the procedure are enhanced by integrating modern techniques like coblation, which minimise tissue trauma and reduce postoperative risks. By providing immediate airway improvement, this approach reduces the need for prolonged interventions, ultimately contributing to better clinical outcomes and improved quality of life for affected infants. Furthermore, the technique has been shown to decrease the incidence of PRAEs, delivering significant clinical and operational benefits. These advantages include enhanced patient safety, optimised resource utilisation, improved surgical efficiency, greater patient and family satisfaction, and reduced long-term morbidity.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
MD; final revision, methodology, and data collection; SZ; methodology, idea formulation; AE; methodology and revision; AS; methodology and editing the final draft; AG; data collection; CP: methodology and final revision.
Ethical approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional research editorial boards and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from the parents or legal guardians of all pediatric participants.
Consent to participate
Written informed consent for participation in this research was obtained from the guardians of all patients.
Consent for publication
All authors have reviewed the final manuscript and consent to its publication. Parental or guardian consent for publication of anonymized data was obtained where applicable.
Availability of data and materials
The data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
History
Received: May 26, 2025
Accepted: August 22, 2025
Figures and tables
| Study group | Control group | χ2 | p | |
|---|---|---|---|---|
| n = 25 (%) | n = 25 (%) | |||
| Gender | ||||
| Female | 10 (40%) | 9 (36%) | ||
| Male | 15 (60%) | 16 (64%) | ||
| Median (IQR) | Median (IQR) | Z | p | |
| Age (months) | 18 (13.5-21.5) | 18 (14.5-23) | -0.438 | 0.661 |
| Comorbidities | ||||
| Absent | 16 (64%) | 16 (64%) | ||
| CHD | 2 (8%) | 2 (8%) | 0.286 | 0.963 |
| Neurological | 4 (16%) | 3 (12%) | ||
| Synchronous airway lesion | 3 (12%) | 4 (16%) | ||
| Symptoms and signs | ||||
| Failure to thrive | 9 (36%) | 11 (44%) | 0.333 | 0.564 |
| Choking | 11 (44%) | 9 (36%) | 0.333 | 0.564 |
| Cyanosis | 4 (16%) | 2 (8%) | Fisher | 0.667 |
| χ 2 : Chi-square test; Z Mann-Whitney test; IQR: interquartile range; CHD: congenital heart disease. | ||||
| Study group | Control group | χ2 | p | |
|---|---|---|---|---|
| n = 25 (%) | n = 25 (%) | |||
| Failure to thrive | ||||
| Preoperative | 9 (36%) | 1 (44%) | 0.333 | 0.564 |
| Postoperative | 1 (4%) | 3 (12%) | Fisher | 0.609 |
| p¥ | 0.008* | 0.008* | ||
| Choking | ||||
| Preoperative | 11 (44%) | 9 (36%) | 0.333 | 0.564 |
| Postoperative | 6 (24%) | 5 (20%) | 0.117 | 0.733 |
| p¥ | 0.063 | 0.125 | ||
| Cyanosis | ||||
| Preoperative | 4 (16%) | 2 (8%) | Fisher | 0.667 |
| Postoperative | 0 (0%) | 1 (4%) | Fisher | > 0.999 |
| p¥ | 0.125 | > 0.999 | ||
| Stridor | ||||
| Preoperative | 25 (100%) | 25 (100%) | Fisher | 0.667 |
| Postoperative | 1 (4%) | 3 (12%) | Fisher | 0.609 |
| p¥ | < 0.001** | < 0.001** | ||
| ¥ p for McNemar test; χ 2 : Chi square test; *p<0.05 is statistically significant; **p ≤ 0.001 is statistically highly significant. | ||||
| Study group | Control group | t | p | |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| Operative time (min) | 17 ± 2.1 | 16.7 ± 2 | 0.543 | 0.59 |
| t: independent sample t-test. | ||||
| Study group (n = 24) | Control group (n = 22) | t | p | |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| Time (days) | 4.8 ± 0.8 | 10.3 ± 1.9 | -11.953 | < 0.001** |
| t: independent sample t-test; **p ≤ 0.001 is statistically highly significant. | ||||
| O2 saturation | Study group (n = 25) | Control group (n = 25) | t | p |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| During sleep | ||||
| Preoperatively | 85.4 ± 4.2 | 86.1 ± 3.2 | -0.706 | 0.484 |
| Postoperatively | 93.7 ± 3.6 | 90.6 ± 3 | 3.268 | 0.002* |
| p§ | < 0.001** | < 0.001** | ||
| While awake | ||||
| Preoperatively | 89.6 ± 3.2 | 91.6 ± 2.8 | -2.355 | 0.023* |
| Postoperatively | 97.4 ± 1.6 | 95.9 ± 2.9 | 2.244 | 0.029* |
| p§ | < 0.001** | < 0.001** | ||
| t: independent sample t-test; § paired sample t-test; **p ≤ 0.001 is statistically highly significant; *p < 0.05 is statistically significant. | ||||
| % change in O2 saturation | Study group (n = 25) | Control group (n = 25) | t | p |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| During sleep | 9.8 ± 3.2 | 5.2 ± 1.4 | 6.423 | < 0.001** |
| Awake | 8.8 ± 3.4 | 4.6 ± 1.3 | 5.622 | < 0.001** |
| t: independent sample t-test; **p < 0.001 is statistically highly significant. | ||||
| Study group | Control group | χ2 | p | |
|---|---|---|---|---|
| n = 25 (%) | n = 25 (%) | |||
| Outcome | ||||
| Failure | 1 (4%) | 3 (12%) | Fisher | 0.609 |
| Success | 24 (96%) | 22 (88%) | ||
| PRAEs | ||||
| Absent | 23 (92%) | 16 (64%) | 5.711 | 0.017* |
| Present | 2 (8%) | 9 (36%) | ||
| χ2: Chi-square test; *p < 0.05 is statistically significant PRAEs perioperative respiratory adverse events. | ||||
References
- Thompson D. Abnormal sensorimotor integrative function of the larynx in congenital laryngomalacia: a new theory of etiology. Laryngoscope. 2007;117:1-33. doi:https://doi.org/10.1097/MLG.0b013e31804a5750
- Landry A, Thompson D. Laryngomalacia: disease presentation, spectrum, and management. Int J Pediatr. 2012;2012. doi:https://doi.org/10.1155/2012/753526
- Walner D, Neumann D, Hamming K. Supraglottoplasty in infants: a staged approach. Ann Otol Rhinol Laryngol. 2015;124:803-807. doi:https://doi.org/10.1177/0003489415585869
- Kay D, Goldsmith A. Laryngomalacia: a classification system and surgical treatment strategy. Ear Nose Throat J. 2006;85:328-336.
- Olney D, Greinwald J, Smith R. Laryngomalacia and its treatment. Laryngoscope. 1999;109:1770-1775. doi:https://doi.org/10.1097/00005537-199911000-00009
- Zalzal G, Anon J, Cotton R. Epiglottoplasty for the treatment of laryngomalacia. Ann Otol Rhinol Laryngol. 1987;96(1 Pt 1):72-76. doi:https://doi.org/10.1177/000348948709600118
- Escher A, Probst R, Gysin C. Management of laryngomalacia in children with congenital syndrome: the role of supraglottoplasty. J Pediatr Surg. 2015;50:519-523. doi:https://doi.org/10.1016/j.jpedsurg.2014.05.035
- El-Kholy N, Hashish M, ElSobki A. Coagulation of the lateral surface of aryepiglottic folds as an alternative to aryepiglottic fold release in management of type 2 laryngomalacia. Auris Nasus Larynx. 2020;47:443-449. doi:https://doi.org/10.1016/j.anl.2019.10.004
- O’Donnell S, Murphy J, Bew S. Aryepiglottoplasty for laryngomalacia: results and recommendations following a case series of 84. Int J Pediatr Otorhinolaryngol. 2007;71:1271-1275. doi:https://doi.org/10.1016/j.ijporl.2007.05.001
- Zheng M, Osterbauer B, Hochstim C. Risk factors for peri-operative respiratory adverse events after supraglottoplasty. Int J Pediatr Otorhinolaryngol. 2021;149. doi:https://doi.org/10.1016/j.ijporl.2021.110853
- Seid A, Park S, Kearns M. Laser division of the aryepiglottic folds for severe laryngomalacia. Int J Pediatr Otorhinolaryngol. 1985;10:153-158. doi:https://doi.org/10.1016/s0165-5876(85)80027-6
- Rosenbek J, Robbins J, Roecker E. A penetration-aspiration scale. Dysphagia. 1996;11:93-98. doi:https://doi.org/10.1007/BF00417897
- Carter J, Rahbar R, Brigger M. International Pediatric ORL Group (IPOG) laryngomalacia consensus recommendations. Int J Pediatr Otorhinolaryngol. 2016;86:256-261. doi:https://doi.org/10.1016/j.ijporl.2016.04.007
- Reinhard A, Gorostidi F, Leishman C. Laser supraglottoplasty for laryngomalacia; a 14 year experience of a tertiary referral center. Eur Arch Otorhinolaryngol. 2017;274:367-374. doi:https://doi.org/10.1007/s00405-016-4252-6
- Daniel S. The upper airway: congenital malformations. Paediatr Respir Rev. 2006;7:S260-S263. doi:https://doi.org/10.1016/j.prrv.2006.04.227
- Richter G, Wootten C, Rutter M. Impact of supraglottoplasty on aspiration in severe laryngomalacia. Ann Otol Rhinol Laryngol. 2009;118:259-266. doi:https://doi.org/10.1177/000348940911800404
- Simons J, Greenberg L, Mehta D. Laryngomalacia and swallowing function in children. Laryngoscope. 2016;126:478-484. doi:https://doi.org/10.1002/lary.25440
- van der Heijden M, Dikkers F, Halmos G. Treatment outcome of supraglottoplasty vs wait-and-see policy in patients with laryngomalacia. Eur Arch Otorhinolaryngol. 2016;273:1507-1513. doi:https://doi.org/10.1007/s00405-016-3943-3
- Bredun S, Kotowski M, Mezydlo J. Characteristics of patients with laryngomalacia: a tertiary referral center experience of 106 cases. Diagnostics (Basel). 2023;13. doi:https://doi.org/10.3390/diagnostics13203180
- Rifai H, Benoit M, El-Hakim H. Secondary airway lesions in laryngomalacia: a different perspective. Otolaryngol Head Neck Surg. 2011;144:268-273. doi:https://doi.org/10.1177/0194599810391600
- Dickson J, Richter G, Meinzen-Derr J. Secondary airway lesions in infants with laryngomalacia. Ann Otol Rhinol Laryngol. 2009;118:37-43. doi:https://doi.org/10.1177/000348940911800107
- Mancuso R, Choi S, Zalzal G. Laryngomalacia. The search for the second lesion. Arch Otolaryngol Head Neck Surg. 1996;122:302-306. doi:https://doi.org/10.1001/archotol.1996.01890150076014
- Krashin E, Ben-Ari J, Springer C. Synchronous airway lesions in laryngomalacia. Int J Pediatr Otorhinolaryngol. 2008;72:501-507. doi:https://doi.org/10.1016/j.ijporl.2008.01.002
- Zwartenkot J, Hoeve H, Borgstein J. Inter-observer reliability of localization of recorded stridor sounds in children. Int J Pediatr Otorhinolaryngol. 2010;74:1184-1188. doi:https://doi.org/10.1016/j.ijporl.2010.07.011
- Bedwell J, Zalzal G. Laryngomalacia. Semin Pediatr Surg. 2016;25:119-122. doi:https://doi.org/10.1053/j.sempedsurg.2016.02.004
- AbdelFattah ElSobki A, Hashish M, El-Kholy N. One and half coblation supraglottoplasty: a novel technique for management of type II laryngomalacia. Int J Pediatr Otorhinolaryngol. 2020;138. doi:https://doi.org/10.1016/j.ijporl.2020.110330
- Ayari-Khalfallah S, Fuchsmann C, Froehlich P. Thulium laser in airway diseases in children. Curr Opin Otolaryngol Head Neck Surg. 2008;16:55-59. doi:https://doi.org/10.1097/MOO.0b013e3282f43419
- Ramprasad V, Ryan M, Farjat A. Practice patterns in supraglottoplasty and perioperative care. Int J Pediatr Otorhinolaryngol. 2016;86:118-123. doi:https://doi.org/10.1016/j.ijporl.2016.04.039
- Timms M, Temple R. Coblation tonsillectomy: a double blind randomized controlled study. J Laryngol Otol. 2002;116:450-452. doi:https://doi.org/10.1258/0022215021911031
- Carney A, Evans A, Mirza S. Radiofrequency coblation for treatment of advanced laryngotracheal recurrent respiratory papillomatosis. J Laryngol Otol. 2010;124:510-514. doi:https://doi.org/10.1017/S0022215109992398
- Ching H, Spinner A, Reeve N. A novel technique for unilateral supraglottoplasty. Int J Pediatr Otorhinolaryngol. 2018;104:150-154. doi:https://doi.org/10.1016/j.ijporl.2017.11.003
- Ayari S, Aubertin G, Girschig H. Pathophysiology and diagnostic approach to laryngomalacia in infants. Eur Ann Otorhinolaryngol Head Neck Dis. 2012;129:257-263. doi:https://doi.org/10.1016/j.anorl.2012.03.005
- Mase C, Chen M, Horn D. Supraglottoplasty for sleep endoscopy diagnosed sleep dependent laryngomalacia. Int J Pediatr Otorhinolaryngol. 2015;79:511-515. doi:https://doi.org/10.1016/j.ijporl.2015.01.018
- El-Sobki A, Ibrahim R, Amer A. Coblation supraglottoplasty: a ten-year experience in a tertiary referral hospital. Eur Arch Otorhinolaryngol. 2022;279:865-874. doi:https://doi.org/10.1007/s00405-021-07130-8
- Eustaquio M, Lee E, Digoy G. Feeding outcomes in infants after supraglottoplasty. Otolaryngol Head Neck Surg. 2011;145:818-822. doi:https://doi.org/10.1177/0194599811414513
- Ramprasad V, Ryan M, Farjat A. Practice patterns in supraglottoplasty and perioperative care. Int J Pediatr Otorhinolaryngol. 2016;86:118-123. doi:https://doi.org/10.1016/j.ijporl.2016.04.039
- Zheng M, Osterbauer B, Hochstim C. Risk factors for peri-operative respiratory adverse events after supraglottoplasty. Int J Pediatr Otorhinolaryngol. 2021;149. doi:https://doi.org/10.1016/j.ijporl.2021.110853
- Schroeder J, Bhandarkar N, Holinger L. Synchronous airway lesions and outcomes in infants with severe laryngomalacia requiring supraglottoplasty. Arch Otolaryngol Head Neck Surg. 2009;135:647-651. doi:https://doi.org/10.1001/archoto.2009.73
- Chan S, Siou G, Welch A. Predictors for routine admission to paediatric intensive care for post-supraglottoplasty laryngomalacia patients. J Laryngol Otol. 2017;131:640-644. doi:https://doi.org/10.1017/S0022215117001074
- Albergotti W, Sturm J, Stapleton A. Predictors of intensive care unit stay after pediatric supraglottoplasty. JAMA Otolaryngol Head Neck Surg. 2015;141:704-709. doi:https://doi.org/10.1001/jamaoto.2015.1033
- Yeung J, Ali S, McKeon M. Carbon dioxide laser versus cold-steel supraglottoplasty: a comparison of post-operative outcomes. Int J Pediatr Otorhinolaryngol. 2020;130. doi:https://doi.org/10.1016/j.ijporl.2019.109843
- Cooper T, Harris B, Mourad A. Comparison between selective and routine intensive care unit admission post-supraglottoplasty. Int J Pediatr Otorhinolaryngol. 2017;99:90-94. doi:https://doi.org/10.1016/j.ijporl.2017.06.001
- Regli A, von-Ungern-Sternberg B. Diagnosis and management of respiratory adverse events in the operating room. Curr Anesthesiol Rep. 2015;5:156-167. doi:https://doi.org/10.1007/s40140-015-0103-z20531171
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 279 times
- PDF downloaded - 63 times