Head and neck
Vol. 46: Issue 2 - April 2026
Subtotal and total glossectomies with or without total laryngectomy – Does laryngeal preservation impact oncological and functional outcomes?
Summary
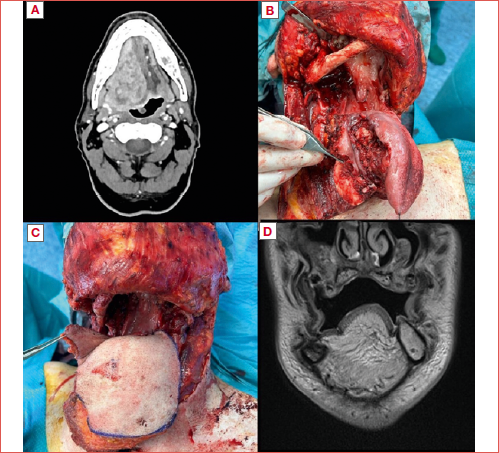
Cover Image
Objective. Subtotal (SG) and total glossectomies (TG) represent surgical options for advanced oral and oropharyngeal squamous cell carcinomas (SCC). Associated laryngeal preservation maintains phonation but increases the risks of aspiration pneumonia and, potentially, local recurrence in the vallecular/supraglottic area. To mitigate these risks, SG/TG with total laryngectomy (TL) may be performed. This study evaluates functional and oncological outcomes of SG/TG with/without TL, focusing on the clinical impact of laryngeal preservation.
Methods. This monocentric retrospective study analysed patients treated by SG/TG with/without TL between January 2013 and July 2024 in a referral, high-volume, academic institution. Oncological outcomes were assessed by overall (OS) and disease-free survival (DFS). Functional outcomes were evaluated in terms of gastrostomy- and tracheotomy-dependency.
Results. Among 67 patients analysed, 56 (83.6%) underwent SG/TG without TL and 11 (16.4%) with TL. Gastrostomy-dependency at discharge was 83.6%, with minimal differences between laryngeal preservation (83.9%) and TL (81.8%). Tracheotomy-dependency in case of laryngeal preservation was 16.7% at 12 months. Five-year OS was 23.1%. No significant differences in terms of OS or DFS were observed between SG/TG with or without TL.
Conclusions. Laryngeal preservation in SG/TG, when oncologically safe, does not worsen survival outcomes and offers better functional recovery. Gastrostomy dependency remains high across both groups, suggesting that laryngeal sacrifice does not confer significant nutritional advantages. State of the art reconstructive techniques using microvascular flaps facilitate laryngeal preservation without compromising survival.
Introduction
Subtotal (SG) and total glossectomies (TG) are first-line treatment options for advanced tongue squamous cell carcinoma (SCC) crossing the midline, typically followed by adjuvant (chemo)radiotherapy [C(RT)], while they should remain as salvage strategies in case of failure of non-surgical therapeutic protocols in advanced oropharyngeal SCC, particularly when bilaterally involving the base of tongue (BOT) 1-4.
Historically, SG and TG with laryngeal preservation have yielded poor functional outcomes, resulting in significant gastrostomy- and tracheotomy-dependency 5. Laryngeal preservation, when oncologically feasible, allows phonation, but increases the risk of aspiration pneumonia with ensuing increased risk of death 6-10. To mitigate these risks, total glosso-laryngectomy (TGL) has been proposed, although its indication is debatable in view of the tremendous impact on the patient’s residual quality of life.
In recent years, advances in reconstructive techniques have led to better functional results 9,10, making SG/TG with laryngeal preservation achievable. Nevertheless, TGL is still performed in selected cases, especially for tumours encroaching the hyoid bone, valleculae and supraglottic region 6,7,11,12. The decision to proceed with SG/TG and total laryngectomy (TL) must carefully consider multiple factors, including patient’s age and comorbidities, tumour extension, and the realistic chance to perform surgery with a curative intent. Even though surgery combined with adjuvant (C)RT has demonstrated therapeutic effectiveness for advanced oral tongue SCC or in salvage scenarios for BOT cancer, the functional impact and quality of life after these procedures must be carefully evaluated. Furthermore, oncological outcomes remain poor in spite of considerable morbidity and potential mortality. The 5-year overall survival (OS) rates reported after SG/TG with TL are approximately 20-35% 6,12-17, being even worse in a salvage setting 18. The lack of long-term survival data limits the understanding of functional outcomes after SG/TG with or without TL. Consequently, in advanced oral and oropharyngeal SCC, the decision to preserve the larynx remains controversial.
The aim of our study was to assess functional and oncological outcomes of SG/TG with or without TL, with a particular focus on determining the clinical impact of laryngeal sacrifice.
Materials and methods
A retrospective single-centre study was conducted at the Department of Otorhinolaryngology – Head and Neck Surgery of Spedali Civili of Brescia, University of Brescia, School of Medicine, Italy, from January 2013 to July 2024. Inclusion criteria were: a) diagnosis of oral and/or oropharyngeal SCC (primary or recurrent); b) surgical treatment including SG/TG with or without concurrent TL; c) treatment with curative intent.
To define SG and TG we employed the classification proposed by Ansarin et al. 19. SGs were categorised as type IVa (anterior SG with preservation of both sides of the BOT) and IVb (i.e. type IVa with extension to one side of the BOT). TGs were classified as type V, involving resection of the entire mobile tongue with the BOT transected at the level of the valleculae. TL was performed only for oncological reasons, when the tumour extended to the hyoid bone, valleculae, or supraglottis, in order to obtain negative margins.
Patients without available follow-up were excluded. Data on patient characteristics, surgical and adjuvant treatment(s), histological details, postoperative complications, and functional and oncological outcomes were anonymously collected in a specific database. Postoperative complications were categorised according to the Clavien-Dindo classification 20. Functional outcomes were assessed as the presence of percutaneous endoscopic gastrostomy (PEG) tube (or any form of artificial enteral feeding) and tracheotomy at hospital discharge, and at 6, 12, and 36 months postoperatively. The Functional Oral Intake Scale (FOIS) score21 was used to objectively evaluate swallowing outcomes at discharge, and patients were divided in 2 categories: PEG-dependent (FOIS scores 1 to 3) and with sufficient oral feeding without a PEG in place (FOIS scores 4 to 7). Oncological outcomes were evaluated in terms of time and status of last follow-up, site, and time of recurrences.
The primary aims of this study were the analysis of oncological outcomes and definition of major prognosticators. Endpoints were 5-year OS and disease-free survival (DFS). A secondary aim was to evaluate functional outcomes according to the type of surgical resection performed (SG/TG with/without TL). Endpoints were PEG- (or any form of artificial enteral feeding) and tracheotomy-dependency. For the latter outcome, patients who underwent concurrent TL were excluded from the analysis.
Statistical analysis
We report values as means with range for descriptive purposes. Categorical variables were compared between different groups using Chi-squared test and Fisher’s exact test. A survival analysis expressed in months was conducted using Kaplan-Meier curves to evaluate oncological outcomes and possible differences between SG/TG with vs. without TL across two main endpoints: OS and DFS. To assess statistical significance, a log-rank test was performed for each endpoint. A p < 0.05 was considered statistically significant.
Results
Patient characteristics
The study population included 67 patients, 42 (62.7%) of whom were males. Mean age at surgery was 63.8 years (range, 40-89). Most of our patients had a primary tumour (67.2%), while the remaining 32.8% had a persistence or recurrence of previously treated lesions. Among the latter, the majority had a history of concomitant CRT. The primary tumour originated in the oral cavity in 82% (n = 55) and oropharynx in 18% (n = 12) of cases. Clinical or radiological involvement of BOT was reported in 34 patients (50.7%). All details are summarised in Table I.
Treatment characteristics and histopathological examinations
The indications to perform TGL rather than SG/TG with laryngeal preservation was related to tumour extension. According to the Ansarin et al. classification 19, in 23.9% of patients the BOT was bilaterally preserved (type IVa SG), in 32.9% only on one side (type IVb SG), and in 26.8% the BOT was bilaterally removed (type V TG). Laryngeal preservation was achieved in 56 (83.6%) patients, while the remaining 16.4% underwent TGL. Other surgical extensions included the tonsil or lateral wall of the oropharynx in 34 (50.7%) cases, buccal mucosa in 9 (13.4%), and alveolar crest mucosa in 14 (20.9%). Segmental and marginal mandibulectomy were performed in 8.9% (n = 6) and 23.9% (n = 16) of patients, respectively (Cover figure).
Neck dissection was performed in almost all patients (97%). Negative surgical margins (R0) were achieved in 82.1% of patients, while the remainder (n = 12), represented exclusively by SG/TG without TL, had microscopical positive margins (R1). In only 2 cases was R1 at the level of valleculae. All defects were reconstructed with a flap: most commonly with a free flap (92.5%), in particular the anterolateral tight (ALTFF) and latissimus dorsi free flaps (LDFF), while a pectoralis major myocutaneous flap was chosen in only 7.5% of cases.
On the basis of the final histological report and multidisciplinary team evaluation, adjuvant treatments were administered to 68.6% (n = 46) of patients, half receiving only RT and the others concurrent CRT. All details are reported in Table II.
Postoperative complications
Mean hospitalisation time was 38.4 days (range, 10-203): 28.6 for TGL and 40.3 in case of laryngeal preservation. Postoperative complications were reported in 29 patients (43.3%) and among these 26.9% (n = 18) were surgical issues. These included 7 free flap failures (10.4%) requiring reconstruction with a second free flap, 5 oral dehiscences (7.5%), 4 oro-cervical fistulas (6%), one postoperative haemorrhage (1.5%), and one free flap vascular congestion (1.5%) salvaged by revision of venous anastomosis.
Medical complications mostly consisted of infections, such as pneumonia, and anaemia requiring transfusions. According to the Clavien-Dindo scores 20, 46.9% of patients (n = 15, 13 SG/TG without TL and 2 TGL) with postoperative complications were classified as IIIb and required a second surgical treatment. None had life-threatening complications requiring intensive care or died during postoperative hospitalisation. Further details are summarised in Table III.
Oncological outcomes
Mean follow-up was 18.1 months (range, 1-91): 14.9% of patients (18.2% and 14.3% of SG/TG with and without TL, respectively) died within the first 3 months after surgery. Three patients were lost to follow-up before 1 year. At the last follow-up, 34.4% were alive: 31.4% without evidence of disease (NED), and 3% with disease (AWD). Patients without evidence of disease represented respectively 45.4% and 28.6% of SG/TG with and without TL. All patients AWD were SG/TG without TL. The remaining 61.2% of patients (n = 41) died: 70.7% (n = 29) due to disease (DOD) and 29.3% (n = 12) for other causes (DOC).
Three- and 5-year OS was 38.8% and 23.1%, respectively, with a median survival of 14 months. SG/TG with TL showed an OS of 30.3% both at 3 and 5 years, with a median survival of 12 months. In the SG/TG without TL group, OS was 40.8% at 3 years and 22.3% at 5 years, with a median of 19 months. No statistically significant differences were found in OS between the 2 groups (p = 0.66) (Figs. 1A,B).
During follow-up, 34 (50.7%) patients had a recurrence. Among these, 26 (38.8%) developed a loco-regional recurrence (4 TGL and 22 SG/TG without TL) after a mean of 11.8 months (range, 1-60). Distant metastases occurred in 16 (23.9%) cases (one TGL and 15 SG/TG without TL) after a mean time of 11.2 months (range, 1-47). All details are reported in Table IV. The median DFS of our population was 17 months. At 3 and 5 years, DFS was 42.2% and 27%, respectively: SG/TG without TL demonstrated a longer DFS, with a median of 20 months. Conversely, in the TGL group, the median DFS was notably lower (8 months) (Figs. 1C,D). According to the log-rank test, no statistically significant difference was highlighted in terms of DFS between the 2 groups (p = 0.66).
Tracheotomy-dependency
Excluding patients submitted to TGL, 17 (30.4%) patients managed by SG/TG without TL maintained the tracheotomy at discharge. Treatment of persistence/recurrence had a significant impact on tracheotomy-dependency at discharge (p = 0.04), but not during follow-up. Correlation between postoperative surgical complications and tracheotomy-dependency at discharge was close to statistical significance (p = 0.06). At 6 and 12 months, tracheotomy-dependency was reported in 25.6% (11 of 43 patients alive) and 16.7% (4 of 24 patients alive), respectively. Patients treated by segmental mandibulectomy had a significant higher tracheotomy-dependency rate at 12 months (p = 0.01), a trend that was not observed in cases of marginal mandibulectomy or other surgical extensions. Conversely, tracheotomy-dependency at discharge and during follow-up was not significantly associated with patient age or postoperative adjuvant treatment(s) (p > 0.05). None required a TL due to chronic aspiration. At 3 years, none of the 11 patients who were alive had a tracheotomy. In the group of patients who removed the cannula, mean decannulation time was 32.5 days (range, 7-198). Additional details are reported in Table III.
Enteral feeding
Swallowing outcomes were evaluated in all cases (SG/TG with or without TL). PEG was placed before surgery in 11 cases (16.4%), but did not significantly impact on PEG-dependency at discharge or during follow-up (p > 0.05). At discharge, a PEG was in place in 83.6% (n = 56) of patients, 81.8% and 83.9% of SG/TG with and without TL, respectively. Postoperative oral feeding was achievable only in 11 (16.4%) patients: 3 had a single consistency oral diet (FOIS score 4) and 8 had a multiple consistency oral diet requiring special preparation (FOIS score 5). None had an exclusive oral diet without or with few limited restrictions (FOIS score 6-7) (p = 0.15). At 6 months, PEG-dependency was reported in 85.1% of patients (40 of 47 alive), and 75% and 86% of SG/TG with and without TL were alive, respectively. At 12 months, patients with PEG represented 65.5% (19 of 29 patients alive): 75% SG/TG with TL and 64% without TL. At 3 years, 3 of 11 (27.3%) patients who were alive had a PEG. The occurrence of surgical complications was significantly associated with PEG-dependency during follow-up (p = 0.02).
On the other hand, older age, persistent/recurrent tumour, and adjuvant treatment(s) were not risk factors for enteral feeding dependency (p > 0.05). Of note, TL was not associated with a higher rate of PEG removal (p > 0.05). In the SG/TG without TL group, no patient required TL due to massive aspiration during follow-up. Additional details are reported in Table III.
Discussion
The analysis of our cohort demonstrated that SG/TG with or without TL were associated with poor survival outcomes, in line with the advanced stages and biologic aggressiveness of these diseases. Moreover, TL does not seem to be associated with higher rates of negative margins or better survival estimates. In terms of functional outcomes, PEG-dependency was remarkable and independent of TL. On the other hand, the decannulation rate in patients without TL was considerable in the long term. Therefore, based on our data, TL should be conceived as an extension of SG/TG to achieve complete tumour resection within R0 margins, and never proposed with the idea of improving functional swallowing outcomes.
Oncological outcomes
Survival rates for advanced oral/oropharyngeal SCC, despite appropriate and aggressive treatment, remain relatively poor. The literature reports a survival rate of 40-50% and 20-35% at one and 5 years, respectively, after SG/TG with or without TL 6,12,13,15-17. OS and DFS in our cohort were, respectively, 38.8% and 42.2% at 3 years, and 23.1% and 27% at 5 years, with a median survival of 14 months and a median DFS of 17 months. Kaplan-Meier curves revealed that survival trajectories after SG/TG with/without TL were largely overlapping across all endpoints (OS, DFS), with no significant differences (Fig. 1). Our results suggest that laryngeal preservation did not have any detrimental effect on survival, in line with previously reported results in salvage settings 18. Nevertheless, a significant selection bias was present in our cohort, as TGL was performed solely for oncologic indications, therefore resulting in the inclusion of patients with more advanced tumours.
Our series showed a perioperative mortality rate of zero, likely due to the careful selection of young and otherwise reasonably healthy patients. Conversely, recommending such a complex procedure for elderly patients or those with significant comorbidities is ethically and clinically questionable. A comprehensive, multidisciplinary assessment of the surgical indications should carefully weigh the potential oncological benefits against the inherent risks of treatment.
Functional outcomes
SG/TG with or without TL result in significant functional impairments and are typically reserved to advanced primary tongue cancers crossing the midline or as part of salvage treatment for oropharyngeal cancer extensively involving the BOT. In head and neck cancer, the balance between curative outcomes and patient quality of life still remains a major challenge 18,22. The mean age of our population was 63.8 years, supporting the idea that surgery should be considered only for relatively young subjects, who are highly motivated and with strong family support.
Mean hospitalisation time was undoubtedly long for both TGL and SG/TG without TL, but even longer in the latter group, thus highlighting the more complex and prolonged process of swallowing rehabilitation in patients with laryngeal preservation. The shape and size of the new BOT play a vital role in the pharyngeal phase of swallowing and impact the risk of aspiration in case of laryngeal preservation 23-25. For nearly all patients a free flap reconstruction was chosen, with ALTFF and LDFF being the most common options due to their bulkiness and relatively stable volume in the long term.
Functional outcomes were assessed based on PEG- and tracheotomy-dependency at discharge and during follow-up. Preoperative PEG, older age, persistent/recurrent tumour, and adjuvant treatment(s) were not negative prognosticators for PEG-dependency. Conversely, the occurrence of surgical complications was significantly linked to PEG-dependency during follow-up, likely due to delayed swallowing rehabilitation, which reduced the chances of recovery. The literature indicates a wide variability of PEG-dependency rates after SG/TG with or without TL ranging from 0% to 77% 26. In our study, at discharge, 83.6% of patients required PEG, with similar rates observed between those who underwent laryngeal preservation and those who did not. Likewise, after 12 months, PEG-dependency was observed in 65.5% of patients, accounting for 64% of SG/TG without TL alive and 75% of SG/TG with TL. Our results were consistent with studies reporting PEG-dependency rates of 71-77% at one year for SG/TG without TL 5,9,27-29 and 53-67% for TGL 11,18,30. The similar PEG-dependency with and without TL is interesting and supports the concept that TL does not enhance nutritional outcomes, aligning with previously reported results in salvage settings 11,18,31. A possible interpretation of this finding is that, even in case of TL, patients struggle to introduce adequate nourishment via an exclusive oral feeding due to the time-consuming and unrewarding action of swallowing, with enteral feeding remaining essential to complement an adequate caloric intake.
Excluding cases of TGL, we analysed tracheotomy-dependency at discharge and during follow-up. Tracheotomy was always performed during surgery and maintained for a variable period, depending on the patient’s ability to manage secretions. The mean decannulation time was 32.5 days. In our population, tracheotomy-dependency decreased from 30.4% at discharge to 16.7% at 12 months, in line with 15-16% of tracheostomy rate at one year reported in the literature 5,27,28,32. Of note, all patients who were alive at 3 years were successfully decannulated.
Patients treated for a persistence/recurrence were significantly more prone to have tracheotomy-dependency at discharge, but not during follow-up. This could be attributed to previous history of (C)RT in nearly all patients with persistence/recurrence, which adversely affects swallowing rehabilitation and restoration of airway patency 33. In the literature, a negative impact on swallowing has also been described in elderly patients 33,35,36. Conversely, we found that patient age did not influence tracheotomy- and PEG-dependency, probably due to the relatively low mean age of our population.
Moreover, we found that segmental mandibulectomy had a significant negative impact on the tracheotomy rate at 12 months, whereas marginal mandibulectomy and other surgical extensions did not. Mandibular involvement is known to be a poor prognostic indicator, but its functional impact is less well defined 28. Many series have excluded these patients 26,27,37 and Kimata et al. 38 in a group of 30 patients found no significant differences. In our cohort, a reconstructive plate with exclusive soft tissue flap reconstruction was used for almost all patients undergoing segmental mandibulectomy, which probably contributed to exacerbating difficulties in swallowing due to suboptimal chewing, oral management of the bolus, and even more incomplete elevation of the hyoid bone. The impaired movement leads to incomplete closure of the epiglottic vestibule, increasing the risk of penetration and aspiration during swallowing, thus increasing tracheotomy-dependency during follow-up 39.
Overall, our findings strongly discourage the indication to a TGL for purely functional reasons, since we did not find any advantage in swallowing rehabilitation. Interestingly, none of the patients with a preserved larynx required TL during follow-up due to massive inhalation and recurrent aspiration pneumonia.
Limitations of our study include its retrospective and single-centre design, as well as assessment of functional outcomes being limited to simple objective measures (PEG- and tracheotomy-dependency), without considering patients’ subjective quality of life as in a previous work of our group related to compartmental hemitongue surgery 40. Moreover, a larger study population would be necessary to obtain more comprehensive data, especially for longer follow-up periods.
Conclusions
Survival and local control rates, despite appropriate treatment, remain low in both SG/TG with and without TL. However, SG/TG without TL, whenever oncologically feasible, is a safe procedure for a selected group of patients with advanced oral and oropharyngeal SCC. The belief that laryngeal sacrifice may reduce the need of PEG-dependency remains unproven. Laryngeal preservation in SG/TG does not worsen oncological outcomes and offers better functional recovery in terms of tracheotomy-dependency. PEG-dependency rates remained high across both groups, suggesting that laryngeal sacrifice does not confer nutritional advantages. The rate of complications is high and postoperative hospitalisation is lengthy; selection of patients with adequate performance status and family support is essential to avoid treatment-related mortality. Advanced reconstructive techniques, especially applying microvascular reconstructions, play a pivotal role for functional recovery, particularly in terms of management of secretions, leading to a high rate of laryngeal preservation. Future prospective, randomised clinical trials are needed to evaluate the balance between oncological efficacy and functional outcomes, aiming to better identify factors that can negatively impact functional recovery. Inclusion of patient-reported outcomes and quality of life measures will be essential to guide clinical decisions.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
CM, MT, FN, GB: contributed to data collection and statistical analysis; CM, CP: contributed to perform manuscript preparation and final edits and revisions; DM, VR, CM, AP, DL, AG, CP: reviewed, contributed conceptually to the article and approved the submitted version.
Ethical consideration
This study was approved by the Institutional Ethics Committee of the University of Brescia (protocol number 6423). The research was conducted ethically, with all study procedures being performed in accordance with the requirements of the World Medical Association’s Declaration of Helsinki.
Written informed consent was obtained from each patient for study participation and data publication.
History
Received: June 7, 2025
Accepted: October 2, 2025
Figures and tables
Figure 1. Kaplan-Meier curves representing overall (OS) and disease free survival (DFS). A) OS of the entire population; B) Comparison between OS of subtotal and total glossectomy (SG/TG) with/without total laryngectomy (TL) subgroups; C) DFS of the entire population; D) Comparison between DFS of SG/TG with/without TL.
| Total | SG/TG without TL | SG/TG with TL | |
|---|---|---|---|
| (N/%) | (N/%) | (N/%) | |
| Patients | 67 | 56 (83.6%) | 11 (16.4%) |
| Male | 42 (62.7%) | 32 (57.1%) | 10 (90.9%) |
| Female | 25 (37.3%) | 24 (42.9%) | 1 (9.1%) |
| Mean age | 63.8 y | 64.1 y | 62.2 y |
| Primary tumour | 45 (67.2%) | 40 (71.4%) | 5 (45.5%) |
| Recurrence | 22 (32.8%) | 16 (28.6%) | 6 (54.5%) |
| Previous treatment: | |||
| S | 3 (4.5%) | 3 (53.6%) | - |
| S+RT/CRT | 5 (7.4%) | 3 (5.4%) | 2 (18.2%) |
| RT | 4 (6%) | 2 (3.6%) | 2 (18.2%) |
| CRT | 7 (10.4%) | 7 (12.5%) | - |
| NEOADJ CHT + S+ RT/CRT | 2 (3%) | 1 (1.8%) | 1 (9.1%) |
| NEOADJ CHT +CRT | 1 (1.5%) | - | 1 (9.1%) |
| Primary site: | |||
| Oral cavity | 55 (82%) | 51 (91.1%) | 4 (36.4%) |
| Oropharynx | 12 (18%) | 5 (8.9%) | 7 (63.6%) |
| BOT involvement: | |||
| Yes | 34 (50.7%) | 23 (41.1%) | 11 (100%) |
| No | 33 (49.3%) | 33 (58.9%) | - |
| cTNM: | |||
| T3 | 42 (62.7%) | 42 (75%) | - |
| T4a | 23 (34.3%) | 12 (21.4%) | 11 (100%) |
| T4b | 2 (3%) | 2 (3.6%) | - |
| N1 | 12 (18%) | 11 (19.6%) | 1 (9.1%) |
| N2a | 2 (3%) | 1 (1.8%) | 1 (9.1%) |
| N2b | 16 (23.9%) | 15 (26.8%) | 1 (9.1%) |
| N2c | 8 (11.9%) | 6 (10.7%) | 2 (18.2%) |
| N3a | 1 (1.5%) | - | 1 (9.1%) |
| N3b | 8 (11.9%) | 6 (10.7%) | 2 (18.2%) |
| N: number; SG/TG: subtotal and total glossectomy (type IVa, IVb, and V according to the Ansarin classification19); TL: total laryngectomy; S: surgery; RT: radiotherapy; CRT: chemoradiotherapy; NEOADJ CHT: neoadjuvant chemotherapy; BOT: base of the tongue; cTNM: clinical classification according to the TNM 8th Edition. | |||
| Total(n/%) | SG/TG without TL | SG/TG with TL | |
|---|---|---|---|
| (N/%) | (N/%) | (N/%) | |
| Type of surgery (Ansarin’s classification): | |||
| IVa | 16 (23.9%) | 16 (28.6%) | - |
| IVb | 22 (32.9%) | 22 (39.3%) | - |
| V | 18 (26.8%) | 18 (32.1%) | - |
| TGL | 11 (16.4%) | - | 11 (100%) |
| Surgical extension: | |||
| Tonsil/lateral wall of the oropharynx | 34 (50.7%) | 28 (50%) | 6 (54.5%) |
| Buccal mucosa | 9 (13.4%) | 9 (16.1%) | - |
| Alveolar crest | 14 (20.9%) | 11 (19.6%) | 3 (27.3%) |
| Segmental mandibulectomy | 6 (8.9%) | 6 (10.7%) | - |
| Marginal mandibulectomy | 16 (23.9%) | 12 (21.4%) | 4 (36.4%) |
| Reconstruction: | |||
| Free flap | 62 (92.5%) | 52 (92.9%) | 10 (90.9%) |
| Pedicled flap | 5 (7.5%) | 4 (7.1%) | 1 (9.1%) |
| Type of flap: | |||
| ALTFF | 34 (50.7%) | 30 (53.5%) | 4 (36.4%) |
| RFFF | 2 (3%) | 2 (3.6%) | - |
| LDFF | 21 (31.3%) | 15 (26.7%) | 6 (54.5%) |
| LDFF+ STFF | 2 (3%) | 2 (3.6%) | - |
| ALTFF+ FFF | 1 (1.5%) | 1 (1.8%) | - |
| LDFF + FFF | 1 (1.5%) | 1 (1.8%) | - |
| RAM | 2 (3%) | 2 (3.6%) | - |
| PM | 4 (6%) | 3 (5.4%) | 1 (9.1%) |
| Neck dissection: | |||
| Homolateral | 5 (7.7%) | 5 (8.8%) | 2 (18.2%) |
| Bilateral | 60 (92.3%) | 52 (91.2%) | 8 (72.7%) |
| Histological examination | |||
| pTNM: | |||
| T3 | 41 (61.2%) | 41 (73.2%) | - |
| T4a | 26 (38.8%) | 15 (26.8%) | 11 (100%) |
| N1 | 4 (6%) | 3 (5.4%) | 1 (9.1%) |
| N2b | 3 (3%) | 3 (5.4%) | - |
| N2c | 1 (1.5%) | 1 (1.8%) | - |
| N3b | 37 (55.2%) | 31 (55.4%) | 6 (54.5%) |
| Grade: | |||
| G1 | 5 (7.7%) | 4 (7.1%) | 1 (9.1%) |
| G1-G2 | 1 (1.5%) | 1 (1.8%) | - |
| G2 | 26 (38.8%) | 22 (39.3%) | 4 (36.4%) |
| G2-G3 | 8 (11.9%) | 6 (10.7%) | 2 (18.1%) |
| G3 | 27 (40.3%) | 23 (41.1%) | 4 (36.4%) |
| Lv1 | 47 (70.2%) | 39 (69.6%) | 8 (72.7%) |
| Pn1 | 62 (92.5%) | 51 (91.1%) | 11 (100%) |
| R: | |||
| R0 | 43 (64.2%) | 34 (60.7%) | 9 (81.8%) |
| R close | 12 (17.9%) | 10 (17.9%) | 2 (18.2%) |
| R1 | 12 (17.9%) | 12 (21.4%) | - |
| Invasion of: | |||
| BOT | 33 (49.3%) | 22 (39.3%) | 11 (100%) |
| Tip of the tongue | 40 (59.7%) | 38 (67.9%) | 2 (18.2%) |
| Tonsil/lateral wall of oropharynx | 16 (23.9%) | 12 (21.4%) | 4 (36.4%) |
| Buccal mucosa | 4 (6%) | 4 (7.1%) | - |
| Mandible | 9 (13.4%) | 8 (14.2%) | 1 (9.1%) |
| Alveolar crest | 2 (3%) | 2 (3.6%) | - |
| Adjuvant therapy: | |||
| RT | 23 (34.3%) | 18 (46.2%) | 5 (45.5%) |
| CRT | 23 (34.3%) | 21 (53.8%) | 2 (18.2%) |
| N: number; SG/TG: subtotal and total glossectomy (type IVa, IVb, and V according to the Ansarin classification19); TL: total laryngectomy; ALTFF: anterolateral tight free flap, RFFF: radial forearm free flap; LDFF: latissimus dorsi free flap; STFF: scapular tip free flap; FFF: fibula free flap; RAM: rectus abdominis myocutaneous flap; PM: pectoralis major flap; pTNM: pathological classification according to the TNM 8th Edition; G1: low grade; G2: intermediate grade; G3: high grade; Lvi: lympho-vascular invasion; Pni: perineural invasion; R: margins status; BOT: base of the tongue; RT: radiotherapy; CRT: chemoradiotherapy. | |||
| Total | SG/TG without TL | SG/TG with TL | |
|---|---|---|---|
| (N/%) | (N/%) | (N/%) | |
| Postoperative complications | 29 patients | 27 patients | 2 patients |
| (43.3%) | (48.2%) | (18.2%) | |
| Surgical complications: | 18 (26.9%) | 16 (28.6%) | 2 (18.2%) |
| Flap failure | 7 (10.4%) | 5 (8.9%) | 2 (18.2%) |
| Flap vascular congestion | 1 (1.5%) | 1 (1.8%) | - |
| Oro-cervical fistula | 4 (6%) | 4 (7.1%) | - |
| Oral dehiscence | 5 (7.5%) | 5 (8.9%) | - |
| Haemorrhage | 1 (1.5%) | 1 (1.8%) | - |
| Medical complications: | 14 (20.9%) | 14 (25%) | - |
| Anaemia | 6 (8.9%) | 6 (10.7%) | - |
| Pneumonia | 5 (7.5) | 5 (8.9%) | - |
| Clostridium colitis | 1 (1.5%) | 1 (1.8%) | - |
| Cardiac failure | 1 (1.5%) | 1 (1.8%) | - |
| Fall-related ulnar fracture | 1 (1.5%) | 1 (1.8%) | - |
| Clavien-Dindo score*: | |||
| I | 4 (6%) | 4 (7.1%) | - |
| II | 10 (14.9%) | 10 (17.8%) | - |
| IIIa | - | - | - |
| IIIb | 15 (22.4%) | 13 (23.2%) | 2 (18.2%) |
| IV | - | - | - |
| V | - | - | - |
| Tracheotomy: | |||
| Definitive (TGL) | 11 (16.4%) | - | 11 (16.4%) |
| At discharge | 17 (30.3%) | 17 (30.3%) | - |
| At 6 months | 11/43 alive (25.6%) | 11/43 alive (25.6%) | - |
| At 12 months | 4/24 alive (16.7%) | 4/24 alive (16.7%) | - |
| At 36 months | 0 /11 alive (0%) | 0 /11 alive (0%) | - |
| PEG/enteral feeding: | |||
| At discharge | 56 (83.6%) | 47 (83.9%) | 9 (81.8%) |
| At 6 months | 40/47 alive (85.1%) | 37/43 alive (86%) | 3/4 alive (75%) |
| At 12 months | 19/29 alive (65.6%) | 16/25 alive (64%) | 3/4 alive (75%) |
| At 36 months | 3 /12 alive (25%) | 3/11 (27.3%) | 0/1 alive (0%) |
| FOIS SCORE at discharge**: | |||
| 1 | 47 (70.1%) | 41 (73.2%) | 6 (54.5%) |
| 2 | 6 (9%) | 3 (5.4%) | 3 (27.3%) |
| 3 | 3 (4.5%) | 3 (5.4%) | - |
| 4 | 3 (4.5%) | 2 (3.6%) | 1 (9.1%) |
| 5 | 8 (11.9%) | 7 (12.5%) | 1 (9.1%) |
| 6 | - | - | - |
| 7 | - | - | - |
| N: number; SG/TG: subtotal and total glossectomy (type IVa, IVb, and V according to the Ansarin classification 19 ); TL: total laryngectomy; PEG: percutaneous endoscopic gastrostomy gastrostomy tube; TGL: total glossolaryngectomy; *Clavien-Dindo score 5 categories 20 : Grade I - Any deviation from the normal postoperative course without the need for pharmacological treatment or interventions; Grade II - Requiring pharmacological treatment with drugs; Grade IIIa - Requiring intervention not under general anesthesia; Grade IIIb - Requiring intervention under general anaesthesia; Grade IVa - Life-threatening complication requiring ICU management with single organ dysfunction; Grade IVb - Life-threatening complication requiring ICU management with multiorgan dysfunction; Grade V - Death; **FOIS score at discharge reported 7 categories 21 : 1) PEG-tube dependent; 2) PEG with minimal/inconsistent oral intake; 3) PEG with consistent oral intake; 4) Total oral intake of a single consistency; 5) Total oral intake of multiple consistencies requiring special preparation; 6) Total oral intake with limited restrictions; 7) Total oral intake with no restrictions. | |||
| Total | SG/TG without TL | SG/TG with TL | |
|---|---|---|---|
| (N/%) | (N/%) | (N/%) | |
| Mean follow-up | 18.1 months | 19.7 months | 15.2 months |
| Dead in the first 3 months after surgery | 10 (14.9%) | 8 (14.3%) | (18.2%) |
| Status at the last follow-up: | |||
| NED | 21 (31.4%) | 16 (28.6%) | 5 (45.4%) |
| AWD | 2 (3%) | 2 (3%) | - |
| DOD | 29 (43.3%) | 26 (46.4%) | 3 (27.3%) |
| DOC | 12 (17.9%) | 9 (16.1%) | 3 (27.3%) |
| LOST | 3 (4.5%) | 3 (5.4%) | - |
| Recurrence during follow-up | 34 (50.7%) | 29 (51.8%) | 5 (45.5%) |
| Local recurrence | 19 (28.4%) | 17 (30.4%) | 2 (18.2%) |
| Regional recurrence | 13 (19.4%) | 11 (19.6%) | 2 (18.2%) |
| Distant recurrence | 16 (23.9%) | 15 (26.8%) | 1 (9.1%) |
| N: number; SG/TG: subtotal and total glossectomy (type IVa, IVb, and V according to the Ansarin classification 19 ); TGL: total glossolaryngectomy; NED: alive without evidence of disease; AWD: alive with disease; DOD: dead of disease; DOC: dead of other cause; LOST: lost to follow-up. | |||
References
- Piazza C, Montalto N, Paderno A. Is it time to incorporate ’depth of infiltration’ in the T staging of oral tongue and floor of mouth cancer?. Curr Opin Otolaryngol Head Neck Surg. 2014;22:81-89. doi:https://doi.org/10.1097/MOO.0000000000000038
- Piazza C, Grammatica A, Montalto N. Compartmental surgery for oral tongue and floor of the mouth cancer: oncologic outcomes. Head Neck. 2019;41:110-115. doi:https://doi.org/10.1002/hed.25480
- Calabrese L, Tagliabue M, Grammatica A. Compartmental tongue surgery for intermediate-advanced squamous cell carcinoma: a multicentric study. Head Neck. 2023;45:2862-2873. doi:https://doi.org/10.1002/hed.27517
- Gazzini L, Dallari V, Caselli A. Modular anatomic approach to oral tongue carcinoma: functional outcomes and quality of life. Acta Otorhinolaryngol Ital. 2024;44:285-295. doi:https://doi.org/10.14639/0392-100X-N3041
- Keski-Säntti H, Bäck L, Lassus P. Total or subtotal glossectomy with laryngeal preservation: a national study of 29 patients. Eur Arch Otorhinolaryngol. 2018;275:191-197. doi:https://doi.org/10.1007/s00405-017-4789-z
- Burnham A, Boyce B, Kaka A. Survival and functional outcomes after total glossectomy with total laryngectomy: case series from a high-volume tertiary institution. Oral Oncol. 2023;137. doi:https://doi.org/10.1016/j.oraloncology.2022.106301
- Razack M, Sako K, Bakamjian V. Total glossectomy. Am J Surg. 1983;146:509-511. doi:https://doi.org/10.1016/0002-9610(83)90242-8
- Sinclair C, Carroll W, Desmond R. Functional and survival outcomes in patients undergoing total glossectomy compared with total laryngoglossectomy. Otolaryngol Head Neck Surg. 2011;145:755-758. doi:https://doi.org/10.1177/0194599811412724
- Longo B, Pagnoni M, Ferri G. The mushroom-shaped anterolateral thigh perforator flap for subtotal tongue reconstruction. Plast Reconstr Surg. 2013;132:656-665. doi:https://doi.org/10.1097/PRS.0b013e31829acf84
- Ferrari M, Sahovaler A, Chan H. Scapular tip-thoracodorsal artery perforator free flap for total/subtotal glossectomy defects: case series and conformance study. Oral Oncol. 2020;105. doi:https://doi.org/10.1016/j.oraloncology.2020.104660
- Lin D, Yarlagadda B, Sethi R. Long-term functional outcomes of total glossectomy with or without total laryngectomy. JAMA Otolaryngol Head Neck Surg. 2015;141:797-803. doi:https://doi.org/10.1001/jamaoto.2015.1463
- Han A, Kuan E, Mallen-St Clair J. Total glossectomy with free flap reconstruction: twenty-year experience at a tertiary medical center. Laryngoscope. 2019;129:1087-1092. doi:https://doi.org/10.1002/lary.27579
- Vartanian J, Magrin J, Kowalski L. Total glossectomy in the organ preservation era. Curr Opin Otolaryngol Head Neck Surg. 2010;18:95-100. doi:https://doi.org/10.1097/MOO.0b013e3283376c3f
- Weber R, Ohlms L, Bowman J. Functional results after total or near total glossectomy with laryngeal preservation. Arch Otolaryngol Head Neck Surg. 1991;117:512-515. doi:https://doi.org/10.1001/archotol.1991.01870170058013
- Barry B, Baujat B, Albert S. Total glossectomy without laryngectomy as first-line or salvage therapy. Laryngoscope. 2003;113:373-376. doi:https://doi.org/10.1097/00005537-200302000-00031
- Bova R, Cheung I, Coman W. Total glossectomy: is it justified?. ANZ J Surg. 2004;74:134-138. doi:https://doi.org/10.1046/j.1445-2197.2004.02912.x
- van Lierop A, Basson O, Fagan J. Is total glossectomy for advanced carcinoma of the tongue justified?. S Afr J Surg. 2008;46:22-25.
- Mazerolle P, Fuchsmann C, Schultz P. Salvage total glossectomy and total glosso-laryngectomy: are they worth it? A GETTEC French multicenter study. Oral Oncol. 2022;130. doi:https://doi.org/10.1016/j.oraloncology.2022.105896
- Ansarin M, Bruschini R, Navach V. Classification of GLOSSECTOMIES: proposal for tongue cancer resections. Head Neck. 2019;41:821-827. doi:https://doi.org/10.1002/hed.25466
- Clavien P, Barkun J, de Oliveira M. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250:187-196. doi:https://doi.org/10.1097/SLA.0b013e3181b13ca2
- Crary M, Mann G, Groher M. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch Phys Med Rehabil. 2005;86:1516-1520. doi:https://doi.org/10.1016/j.apmr.2004.11.049
- Windon M, Le D, D’Souza G. Treatment decision-making among patients with oropharyngeal squamous cell cancer: a qualitative study. Oral Oncol. 2021;112. doi:https://doi.org/10.1016/j.oraloncology.2020.105044
- Bhattacharya S, Thankappan K, Joseph S. Volume and location of the defect as predictors of swallowing outcome after glossectomy: correlation with a classification. Dysphagia. 2021;36:974-983. doi:https://doi.org/10.1007/s00455-020-10224-w
- Urken M, Moscoso J, Lawson W. A systematic approach to functional reconstruction of the oral cavity following partial and total glossectomy. Arch Otolaryngol Head Neck Surg. 1994;120:589-601. doi:https://doi.org/10.1001/archotol.1994.01880300007002
- Shukla V. Reconstruction of sub-total and total glossectomy defects: an arduous challenge. Indian J Otolaryngol Head Neck Surg. 2023;75:2643-2644. doi:https://doi.org/10.1007/s12070-023-03843-w
- Dziegielewski P, Ho M, Rieger J. Total glossectomy with laryngeal preservation and free flap reconstruction: objective functional outcomes and systematic review of the literature. Laryngoscope. 2013;123:140-145. doi:https://doi.org/10.1002/lary.23505
- Rihani J, Lee M, Lee T. Flap selection and functional outcomes in total glossectomy with laryngeal preservation. Otolaryngol Head Neck Surg. 2013;149:547-553. doi:https://doi.org/10.1177/0194599813498063
- Rigby M, Hayden R. Total glossectomy without laryngectomy - a review of functional outcomes and reconstructive principles. Curr Opin Otolaryngol Head Neck Surg. 2014;22:414-418. doi:https://doi.org/10.1097/MOO.0000000000000076
- Mazarro A, de Pablo A, Puiggròs C. Indications, reconstructive techniques, and results for total glossectomy. Head Neck. 2016;38:E2004-E2010. doi:https://doi.org/10.1002/hed.24369
- Weyh A, Mosquera C, Nedrud S. Functional outcomes and survival after total glossectomy with laryngectomy: a systematic review. Int J Oral Maxillofac Surg. 2025;54:103-108. doi:https://doi.org/10.1016/j.ijom.2024.07.005
- Kamhieh Y, Fox H, Healy S. Total glossolaryngectomy cohort study (N = 25): survival, function and quality of life. Clin Otolaryngol. 2018;43:1349-1353. doi:https://doi.org/10.1111/coa.13121
- Demir U, Aslıer M, İnan H. Comparison of treatment outcomes between total and near total glossectomy with larynx preservation and flap reconstruction: a single institution experience with 23 patients. Turk Arch Otorhinolaryngol. 2022;60:72-79. doi:https://doi.org/10.4274/tao.2022.2022-4-1
- Russo E, Alessandri-Bonetti M, Costantino A. Functional outcomes and complications of total glossectomy with laryngeal preservation and flap reconstruction: a systematic review and meta-analysis. Oral Oncol. 2023;141. doi:https://doi.org/10.1016/j.oraloncology.2023.106415
- Smith J, Suh J, Erman A. Risk factors predicting aspiration after free flap reconstruction of oral cavity and oropharyngeal defects. Arch Otolaryngol Head Neck Surg. 2008;134:1205-1208. doi:https://doi.org/10.1001/archotol.134.11.1205
- Borggreven P, Verdonck-de Leeuw I, Rinkel R. Swallowing after major surgery of the oral cavity or oropharynx: a prospective and longitudinal assessment of patients treated by microvascular soft tissue reconstruction. Head Neck. 2007;29:638-647. doi:https://doi.org/10.1002/hed.20582
- Miyamoto S, Sakuraba M, Nagamatsu S. Risk factors for gastric-tube dependence following tongue reconstruction. Ann Surg Oncol. 2012;19:2320-2326. doi:https://doi.org/10.1245/s10434-012-2298-2
- Navach V, Zurlo V, Calabrese L. Total glossectomy with preservation of the larynx: oncological and functional results. Br J Oral Maxillofac Surg. 2013;51:217-223. doi:https://doi.org/10.1016/j.bjoms.2012.07.009
- Kimata Y, Uchiyama K, Ebihara S. Postoperative complications and functional results after total glossectomy with microvascular reconstruction. Plast Reconstr Surg. 2000;106:1028-1035. doi:https://doi.org/10.1097/00006534-200010000-00012
- Ibrahim A, Elgamal M, Abdel-Khalek E. Hyoid displacement during swallowing function for completely edentulous subjects rehabilitated with mandibular implant retained overdenture. BMC Oral Health. 2024;24. doi:https://doi.org/10.1186/s12903-024-04616-9
- Grammatica A, Piazza C, Montalto N. Compartmental surgery for oral tongue cancer: objective and subjective functional evaluation. Laryngoscope. 2021;131:E176-E183. doi:https://doi.org/10.1002/lary.28627
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 607 times
- PDF downloaded - 167 times