Reviews
Vol. 46: Issue 3 - June 2026
Traumatic lesions of the cervical trachea: conservative or surgical treatment? A systematic review
Summary
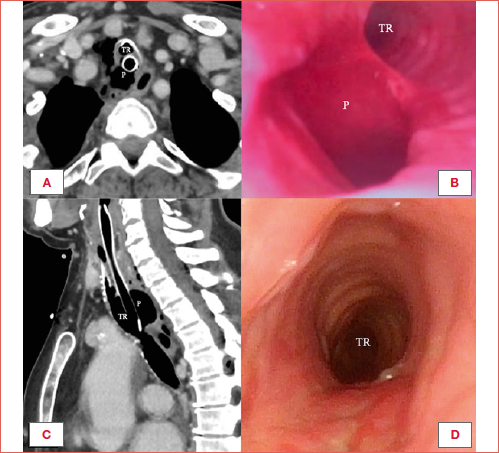
Cover Image
Traumatic lesions of the cervical trachea are rare but critical conditions potentially resulting either from blunt, penetrating, or iatrogenic injuries. These traumatic events pose challenges in airway management due to their life-threatening nature and need for rapid decision-making. Choice of treatment – conservative versus surgical – depends on injury dynamics, features of the traumatic lesion, and patient-related factors. This systematic review, conducted following PRISMA guidelines on 211 studies involving 509 patients, evaluates management strategies, focusing on indications for conservative versus surgical approaches and differences between adults and children. Surgical treatment was preferred for penetrating and severe blunt traumas, while conservative management, such as distal intubation, was used for small, superficial lesions. Surgical indications included tears > 20 mm, significant subcutaneous emphysema, and ventilation failure. Treatment should be individualised based on lesion characteristics and patient factors. Surgery remains essential for severe cases, while conservative approaches are viable in selected scenarios, especially in children.
Introduction
Airway injuries involving the cervical trachea represent a rare but potentially life-threatening occurrence, which may result from either external or endoluminal traumas. The first scenario can be due to penetrating or blunt trauma, while the latter can be the consequence of intubation manoeuvres, long-lasting invasive ventilation, surgical interventions, and - especially in the pediatric population - foreign body ingestion 1. The incidence of tracheal injuries ranges between 0.5 and 2% after blunt trauma 2, growing to 3-6% in penetrating injuries 3.
The management and treatment of these patients is challenging both for the specific anatomical conditions, potentially altered by the trauma itself, and for the quick decision-making process required by such a situation. Clinical presentation and symptoms may vary between spontaneous breath and severe respiratory distress, with patient’s symptoms depending not only on the extent of injury, but also on the presence of concomitant lesions to other organs, such as the oesophagus, cervical spine, and major neck and/or thoracic vessels 4. The first step of the management is always to secure a safe airway (A-management) to allow ventilation without further compromising the laryngotracheal framework. The decision between conservative and surgical treatments should be then discussed considering the patient’s clinical conditions, extent of tracheal damage, and involvement of other structures. Given the challenges in documenting tracheal injuries, stemming from the intrinsic rarity of the condition and its elevated mortality, the literature is lacking specific guidelines and clear indications about whether to proceed with conservative or surgical treatment, and under which circumstances.
Our work finds its place within this context, with the goal of performing a systematic review of the literature on management of traumatic lesions of the cervical trachea, specifically addressing airway management, indications for treatment, and outcomes, aiming to fill the gap in knowledge.
Materials and methods
Objectives
The primary objective was to define the management and treatment of cervical tracheal trauma, with particular focus on the indications of conservative versus surgical approaches. A further objective was to define potential differences in treatment strategies between the adult and paediatric populations (defined as younger than 18 years).
Search strategy
This systematic review follows the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) recommendations. The query “(cervical OR neck) AND trachea* AND (rupture OR laceration OR injury OR trauma OR transection)” was used to make a comprehensive search on PubMed, Scopus, and Web of Science.
Selection criteria
We considered only papers published from January 1st, 2000 to August 26th, 2024, sorted by English language. Book chapters, non-human or autoptic studies, and purely thoracic tracheal traumas were excluded, as well as articles missing sufficient information on both traumatic event and management. All titles and abstracts were screened and full text obtained for selected publications.
Data extraction
Data entry and analysis were carried out and a dedicated database was built. For each study demographic features (age, gender), dynamics of trauma (blunt, penetrating, iatrogenic, spontaneous, foreign body, or resulting from childbirth), clinical presentation (respiratory distress), tracheal wound features (location, size), management (conservative, surgical), and related outcomes were collected.
Lesion size was reported according to its cranio-caudal extension. Conservative management was defined as clinical observation, intubation, and tracheal stent placement, while surgical treatment included tracheotomy, cervical drainage, and airway repair.
Results
The initial search returned 4,783 records. After identification and screening, a total of 211 full text articles, both case series (Tab. I) and case reports 5-176 involving 509 patients, were included in the present review (Fig. 1).
Demographics
The main features of the population are listed in Table II, the majority consisting of adult males, with a mean age of 31 years.
Aetiology
The majority of traumas were due to blunt (n = 220, 43.2%) and penetrating (n = 97, 19.1%) events. Iatrogenic and other types of lesions were reported with lesser incidence. Details are outlined in Table III.
Respiratory distress and first management
At the onset, signs and symptoms of respiratory distress were documented in 153 patients (30.1%). In addition, 83 patients (16.3%) were reported to have airway patency already secured by tracheotomy or intubation at the time of diagnosis. In case of respiratory distress after the traumatic event, the majority of patients were managed directly in the hospital where they were subsequently treated (n = 91, 60%). In other, usually more severe cases, patients were initially managed in field (n = 28, 18%) or local hospitals (n = 23, 15%) before being transferred to the referral centre. In a small percentage of cases, the airway was not managed as an emergency, but restored along with trauma treatment (n = 5, 3.3%), while in a few cases the patient was already intubated (n = 3, 1.9%) or on extracorporeal membrane oxygenation (n = 1, 0.7%). Airway management in case of respiratory distress is outlined in Table IV.
Management
The data compares conservative, surgical, and tracheotomy approaches across the paediatric and adult populations. In the paediatric group (n = 105), conservative methods were described in 34 cases (32.3%), surgical interventions in 64 (61%), and tracheotomy alone in 7 (6.7%). Among the adult population (n = 378), conservative management accounted for 47 cases (12.4%), while surgical approaches were 315 (83.3%), and tracheotomy alone was performed in 15 cases (3.9%). Additionally, there were 26 surgical cases in which patient’s age was not specified. One patient died shortly after the diagnosis.
Among 81 patients treated conservatively, 36 (44.4%) underwent exclusive clinical monitoring (n = 23, 48.9% adults and n = 13, 38.2% children), while 27 (33.3%) were intubated (n = 9, 19.1% adults and n = 18, 52.9% children). In the adult series, 6 patients (7.4%) underwent tracheal stent placement only. These data were not available in 12 cases. In the conservatively treated group, the mean lesion length was 18.1 mm, while among the patients treated with exclusive clinical monitoring the average lesion size was 15 mm in both populations. Intubated children presented lesions with an average size of 13.6 mm, while in adults the average lesion size was 25.2 mm.
Most of the surgically treated patients underwent airway repair (n = 405, 94.9%), while few patients were only tracheotomised (n = 22, 5.1%). Different types of surgical repair are outlined in Table V.
Among surgically treated patients, the average lesion size was 24.7 mm in adults and 30.5 mm in children, while patients that received a tracheotomy alone had an average lesion size of 31.6 mm in adults and 21.7 mm in children. In the computation of the average dimensions, cases of crico-tracheal separation (n = 12 in children and n = 49 in adults) and complete tracheal separation (n = 10 in children and n = 9 in adults) were not considered. All patients with this type of trauma, however, underwent surgical treatment.
Overall, after surgical treatment, an endotracheal stent was applied in 21 cases (5.2%): 6 after primary closure (5.7%) in the adult population, in 12 cases after tracheo-tracheal or laryngo-tracheal anastomosis (n = 8 adults, 4.8% and n = 4 children, 14.8%), 2 cases after laryngo-tracheal reconstruction in children (50%), and after local muscle flap suture in an adult (9%).
In 17 cases (4.2%) the use of muscular flap was reported in association with tracheal repair: 8 cases (n = 5 adults and n = 3 children) after tracheal wound closure, and 9 (n = 5 adults and n = 4 children) as reinforcement of the anastomosis. The muscles used both as support for closure or as a stand-alone repair technique were the prelaryngeal (n = 24, 80%), the sternocleidomastoid (n = 5, 16.7%), and the platysma (n = 1, 3.3%).
In the management of tracheo-oesophageal fistulas, other flaps were used either alone or in combination with muscles as interposition between the oesophagus and trachea: fascia lata (n = 4), colon (n = 3), and a single case of pericardial flap.
Overall, 32% of patients (n = 102 adults and n = 28 children) required tracheostomy after surgery.
Outcomes
Mean follow-up lasted 12.6 months (range, 18 days – 5 years). As a consequence of the trauma, some patients reported unilateral (n = 11, 2.2%) or bilateral (n = 17, 3.3%) vocal cord paralysis.
Analysis of treatment outcomes in adults and children revealed distinct patterns across conservative and surgical managements. Among adults, conservative treatment (n = 47) resulted in stenosis in 4.3% and death in 4.3% of cases. In children who underwent conservative treatment (n = 34), a late stenosis occurred in 25.7%. In the population who received tracheotomy alone, among the adult cohort (n = 15), 6.7% died after the event, while in children (n = 7) a late stenosis was observed in 42.9% of cases. Surgical intervention in adults (n = 315) and children (n = 64), was associated to postoperative stenosis in 2.9% and 1.6% of cases, respectively, tracheo-oesophageal fistula in 1.3% of adults, and death rates of 1% in adult and 7.9% in children, respectively.
Subsequent tracheotomy removal was performed in 35 patients (n = 29 adults and n = 6 children), resulting in an overall decannulation rate of 26.9%. Patients in whom decannulation was not possible were those who required prolonged ventilation due to spinal cord injuries, suffering from bilateral vocal cord paralysis or presenting recurrent stenosis.
Among the 22 patients treated with tracheotomy alone, the overall decannulation rate was 63.6% (n = 8 adults and n = 6 children). In the adult population the average decannulation time was 3.1 months (range, 5 days – 1 year), while in children it was 2.5 months (range, 10 days – 6 months).
Discussion
Tracheal trauma is a rare but potentially life-threatening event that must be diagnosed and treated as quick as possible, since time of management and good functional outcomes are strictly linked. The literature lacks a clear consensus on type of management, airway stabilisation method and treatment, in both the paediatric and adult populations. In such a scenario, our systematic review aims to fill a gap in the accumulated evidence, due to the sparse experience that even large, referral centres for airway disease may accumulate in several years of practice.
Demographic features and aetiology
Males are more affected than females both in the paediatric and adult populations 177. Blunt and penetrating traumas still represent the most common causes of tracheal injury, with a prevalence of the former especially in the paediatric population. This trend confirms the general incidence reported in the literature for cervical and laryngeal traumas, in which there is an increasing number of penetrating lesions with respect to blunt injuries that are probably prevented by the growing use of increasingly safe systems 178,179.
Management
There is no consensus regarding initial airway management when laryngo-tracheal trauma is suspected, as clinical presentation depends on the extension of the injury as well as on the complexity of the patient, considering the high probability of lesions in other areas of the body. Furthermore, it is important to balance the need to secure the airway with the possibility of worsening the injury or creating a false path 23.
Our review shows that most of the patients with respiratory distress at the onset were stabilised through orotracheal intubation at the referral centre. This is a safe technique when performed under visual guidance (e.g. flexible bronchoscope) by expert physicians; however, when a quick endotracheal intubation is performed blindly, it may worsen tracheal injury by creating false passages of the tube, dislocating fractured cartilages, or even leading to airway transection 3. In our analysis, tracheotomy was used as the first choice for airway stabilisation in patients with respiratory distress in 28% of cases.
Conservative management
The present literature review outlines that conservative treatment can be considered in very specific scenarios, especially in the paediatric population 59,180. In this small cohort of patients, in fact, almost half of traumas are represented by contusive neck injury (typically, neck against bicycle handlebars) that may cause small tears in the membranous part of the trachea, without involvement of the oesophagus. If the injury did not cause an immediate airway issue, as a respiratory distress in the most severe cases or an expanding emphysema, conservative treatment can be considered. This often happens with small and/or superficial lesions. In fact, the average dimension of the tracheal tears reported in the cohort of patients who were selected for conservative treatment was 18.1 mm, in accordance with the 20 mm cut-off reported by Mullan et al. 59.
Conservative treatment includes both invasive (i.e. after tracheal intubation) and non-invasive clinical monitoring. A prolonged intubation with high volume, low pressure endotracheal cuff inflated distally to the site of the injury may facilitate healing process 128,181-183. In our review, this treatment strategy was chosen more frequently in children. In the scenario of asymptomatic patients with very superficial iatrogenic injuries (grade I and II according to Cardillo et al. 184) (Tab. VI), invasive ventilation could also be avoided.
Use of a stent as unimodal therapy has been described in exceedingly rare cases, predominantly in patients presenting with a heavily compromised clinical status. Its placement offers a rapid but temporary solution, thus rendering it appropriate for patients unable to withstand an immediate surgical repair and its associated risks 32,185. In our personal experience, in fact, tracheal stents might be considered as a temporary solution in order to allow the patient to heal properly in preparation of subsequent surgical procedures, or as a last resort in otherwise untreatable patients.
Surgical management
Surgical treatment appears strongly indicated in patients with extended and/or complete tracheal wall laceration, in which ventilation cannot be safely performed. Patients requiring surgery for lesions of other cervical or thoracic structures (e.g. major vessels), with tracheo-oesophageal fistula, or signs of impending infection, are adequate candidates for surgical repair. In fact, those with penetrating trauma frequently undergo simultaneous surgical treatment of the tracheal lesion during cervical exploration performed to assess and repair other vascular and visceral damages.
In our systematic review, we highlighted that surgical treatment was chosen in cases where the average lesion size was 24.7 mm in adults and 30.5 mm in children, confirming that surgery is preferred over conservative treatment when tracheal tears are larger than 20 mm 59.
The most reported surgical treatment was represented by primary closure of the tracheal tear through an anterior approach achieved via a circumferential tracheal incision followed by a trans-tracheal repair and (crico-)tracheal anastomosis 186,187 (Cover figure). This surgical technique was also used in case of complete laryngo-tracheal separation or tracheal rupture involving > 75% of the tracheal circumference 108,188-190. For small superficial tears, in selected adult patients, and with the appropriate instrumentation, an endoscopic suture has also been described 191.
Few authors described the use of myofascial pedicled flaps (especially from prelaryngeal muscles) as a support/cover for tracheal repair, mainly in case of tracheo-oesophageal fistula 192. There is no consensus in the literature about this technique, which depends mostly on the integrity of muscular tissues after the traumatic event, the size of the lesion, and the surgeon’s preferences.
The use of stents after surgical management is debated. In our review, a minority of authors described the use of endotracheal stents (e.g. Montgomery T-tube or Dumon) to prevent tracheal stenosis and facilitate the healing process 193. Where described, the issues related to the use of stents, especially T-tubes, are also evident, such as obstruction of the upper limb caused by granulation tissue, tracheal and laryngeal mucosa irritation caused by stent movements, as well as the need for frequent cleaning to prevent secretion drying and subsequent airway blockage 194.
Outcomes
Overall, outcomes assessed in this population were poorly described. According to the available data, a non-negligible number of complications occurred more frequently in conservatively treated patients, particularly children 183. Despite the limited number of cases documented in the literature, a high incidence of stenosis (42.9%) was also observed in paediatric patients who underwent tracheostomy without subsequent tracheal injury surgical repair. Among those undergoing tracheostomy, the available data in the literature indicate that the overall decannulation rate after surgery was 26.9%.
Study limitations
Heterogeneity represents the main limit of the present review. This is true for the pathology itself, which is heterogeneous by definition, potentially underestimated and underrated by the overall trauma assessment. The heterogeneity can be also attributed to the preference of management among single institutions, specific surgical expertise, and selection bias. Moreover, not all manuscripts adequately reported clinical findings and treatment outcomes.
Conclusions
Despite the rarity of cervical tracheal trauma and the heterogeneity of its presentation, correlated with both different causes and characteristics, our systematic review highlights the importance of a prompt airway management and the pivotal role of a clear treatment strategy. Conservative approach is adequate in the specific scenarios of tracheal tears with a cranio-caudal length < 20 mm and without respiratory issues, especially in children. In all the other clinical scenarios, surgical options should be considered as the first choice. An adequate follow-up of some months appears indicated also when a conservative treatment strategy has been applied, in order to promptly detect post-traumatic late stenosis to be treated by secondary surgical endoscopic and/or open techniques.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors did not receive any financial support for the research, authorship and publication of this article.
Author contributions
CM, DL, CP: study conception and design, critical revision of the article and final approval of the version to be published; CM, DL: articles search and selection, data acquisition and analysis, review drafting; AS: articles search and selection, data acquisition.
Ethical consideration
No formal ethics committee approval was required for this article as it is based on already published clinical data from other studies available in the literature.
History
Received: July 27, 2025
Accepted: October 6, 2025
Figures and tables
Figure 1. Flow chart according to the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) recommendations.
| Authors | Population | No. of cases | Aetiology | Management | |
|---|---|---|---|---|---|
| 1 | Liu et al. 195 | Adults | 5 | Ventilation | Surgical |
| 2 | Da Silva Costa et al. 186 | Adults | 2 | Intubation | Surgical |
| 3 | Cassada et al. 196 | Adults | 9 | Penetrating (7), blunt (2) | Surgical (8), death (1) |
| 4 | Almasi et al. 197 | Adults and children | 2 | Blunt | Surgical |
| 5 | Ehab Hussein et al. 38 | Adults | 4 | Intubation | Surgical |
| 6 | Evermann et al. 198 | Adults and children | 26 | Intubation (19), foreign body (7) | Surgical |
| 7 | Dong Ye et al. 199 | Adults | 17 | Blunt | Surgical |
| 8 | Wu et al. 200 | Adults and children | 7 | Blunt | Surgical |
| 9 | Cunningham et al. 201 | Children | 2 | Intubation | Conservative |
| 10 | Han et al. 185 | Adults | 2 | Surgery | Conservative |
| 11 | Elbadan et al. 202 | Adults | 23 | Blunt | Surgical |
| 12 | Bin Pervez et al. 203 | Adults | 12 | Penetrating (3), blunt (3), intubation (6) | Surgical |
| 13 | Herrmann et al. 191 | Adults | 50 | Surgery | Surgical |
| 14 | Mubarak et al. 204 | Adults | 50 | Blunt (35), penetrating (15) | Surgical |
| 15 | Frost et al. 205 | Adults | 2 | Intubation, surgery | Conservative |
| 16 | Bowley et al. 188 | Adults and children | 2 | Blunt | Surgical |
| 17 | Yalçın et al. 206 | Children | 6 | Foreign body (4), surgery (2) | Conservative (1), surgical (5) |
| 18 | Duval et al. 181 | Children | 5 | Blunt | Conservative |
| 19 | Chandra et al. 192 | Adults and children | 10 | Foreign body (4), blunt (3), surgery (2), penetrating (1) | Surgical |
| 20 | Li et al. 207 | Children | 6 | Penetrating | Surgical |
| 21 | Carbognani et al. 208 | Adults | 6 | Intubation | Conservative (2), surgical (4) |
| 22 | Hsu et al. 209 | Children | 8 | Blunt (2), intubation (4), surgery (1), ventilation (1) | Conservative (4), surgical (4) |
| 23 | Guo et al. 210 | Adults | 2 | Foreign body | Conservative |
| 24 | Corsten et al. 211 | Children | 2 | Blunt | Surgical |
| 25 | Lyons et al. 189 | Adults and children | 22 | Penetrating | Conservative (1), surgical (21) |
| 26 | Aerni et al. 212 | Adults | 2 | Surgery | Surgical |
| 27 | Kaintura et al. 193 | Adults | 5 | Blunt | Surgical |
| 28 | Łochowski et al. 213 | Adults | 6 | Penetrating | Surgical |
| 29 | Janni et al. 187 | Adults | 3 | Intubation | Surgical |
| 30 | Mazita et al. 214 | Adults | 2 | Blunt | Surgical |
| 31 | Gòmez-Caro Andrés et al. 215 | Adults and children | 9 | Intubation | Conservative (8), surgical (1) |
| 32 | Mahieu et al. 216 | Children | 4 | Intubation (2), Birth (2) | Conservative (1), surgical (3) |
| 33 | Pan et al. 217 | Adults and children | 2 | Penetrating | Surgical |
| 34 | Sippel et al. 182 | Adults | 2 | Intubation | Conservative |
| 35 | Atalay et al. 218 | Adults | 2 | Intubation | Conservative (1), surgical (1) |
| 36 | Seidl et al. 219 | Children | 2 | Foreign body | Surgical |
| 37 | Wood et al. 183 | Children | 7 | Blunt (1), intubation (5), dilatation (1) | Conservative (6), surgical (1) |
| 38 | Leoncini et al. 190 | Adults | 7 | Penetrating (2), blunt (2), intubation (3) | Conservative (5), surgical (2) |
| 39 | Borowski et al. 220 | Adults | 2 | Blunt | Surgical |
| 40 | Huang et al. 194 | Adults | 2 | Penetrating | Conservative |
| Adults | Children | NA | Total | |
|---|---|---|---|---|
| Males | 233 | 61 | 4 | 298 (58.6%) |
| Females | 92 | 44 | 22 | 158 (31%) |
| NA | 53 | - | - | 53 (10.4%) |
| Total | 378 (74.1%) | 105 (20.8%) | 26 (5.1%) | 509 |
| Age, yrs, mean (range) | 40.9 (18-92) | 8.3 (0-17) | 65.7 | 31 |
| NA: not available. | ||||
| Etiology | Adults (n = 378) | Children (n = 105) | NA (n = 26) | ||
|---|---|---|---|---|---|
| Blunt trauma | 194 | 38.1% | 143 (37.9%) | 51 (48.6%) | - |
| Penetrating trauma | 98 | 19.3% | 85 (22.4%) | 13 (12.4%) | - |
| Iatrogenic trauma: surgery | 82 | 16.1% | 77 (20.4%) | 5 (4.8%) | - |
| Iatrogenic trauma: intubation | 80 | 15.7% | 45 (11.9%) | 16 (15.2%) | 19 (73.1%) |
| Iatrogenic trauma: ventilation | 18 | 3.5% | 16 (4.2%) | 2 (1.9%) | - |
| Foreign body | 16 | 3.1% | 5 (1.3%) | 4 (3.8%) | 7 (26.9%) |
| Iatrogenic trauma: dilatation | 11 | 2.2% | 3 (0.8%) | 8 (7.6%) | - |
| Spontaneous | 8 | 1.6% | 4 (1.1%) | 4 (3.8%) | - |
| Childbirth | 2 | 0.4% | - | 2 (1.9%) | - |
| NA: not available. | |||||
| Field | Local hospital | Referral centre | Total | |
|---|---|---|---|---|
| (n = 28) | (n = 23) | (n = 91) | (n = 142) | |
| OT-NT intubation | 16 (57.1%) | 14 (60.9%) | 58 (63.7%) | 88 (62%) |
| Tracheostomy | 8 (28.6%) | 8 (34.8%) | 24 (26.4%) | 40 (28.2%) |
| Wound intubation | 4 (14.3%) | 1 (4.3%) | 7 (7.7%) | 12 (8.4%) |
| ECMO | - | - | 2 (2.2%) | 2 (1.4%) |
| OT: orotracheal; NT: nasotracheal; ECMO: extracorporeal membrane oxygenation. | ||||
| Total | Adults | Children | NA | |
|---|---|---|---|---|
| (n = 405) | (n = 405) | (n = 64) | (n = 26) | |
| Tracheal repair + (C)TRA | 191 (47.2%) | 164 (52.1%) | 27 (42.9%) | - |
| Primary closure NOS | 158 (39%) | 106 (33.7%) | 26 (41.2%) | 26 (100%) |
| Endoscopic repair | 24 (5.9%) | 24 (7.6%) | - | - |
| Muscle flap alone | 13 (3.2%) | 11 (3.5%) | 2 (3.2%) | - |
| Laryngotracheal reconstruction | 6 (1.5%) | 2 (0.6%) | 4 (6.3%) | - |
| Colon interposition | 3 (0.8%) | - | 3 (4.8%) | - |
| Total laryngectomy | 1 (0.3%) | 1 (0.3%) | - | - |
| Cervical drainage insertion | 3 (0.8%) | 2 (0.6%) | 1 (1.6%) | - |
| NA | 7 (1.5%) | 5 (1.6%) | 1 (1.6%) | - |
| (C)TRA: (crico)tracheal resection and anastomosis; NOS: not otherwise specified; NA: not available. | ||||
| Classification | Morphologic description |
|---|---|
| Level I | Mucosal or submucosal tracheal involvement without mediastinal emphysema and without oesophageal injury |
| Level II | Tracheal lesion up to the muscular wall with subcutaneous or mediastinal emphysema without oesophageal injury or mediastinitis |
| Level IIIA | Complete laceration of the tracheal wall with oesophageal or mediastinal soft-tissue hernia without oesophageal injury or mediastinitis |
| Level IIIB | Any laceration of the tracheal wall with oesophageal injury or mediastinitis |
References
- Philteos J, James A, Propst E. Airway complications resulting from pediatric esophageal button battery impaction: a systematic review. JAMA Otolaryngol Head Neck Surg. 2022;148:677-683. doi:https://doi.org/10.1001/jamaoto.2022.0848
- Wong E, Knight S. Tracheobronchial injuries from blunt trauma. ANZ J Surg. 2006;76:414-415. doi:https://doi.org/10.1111/J.1445-2197.2006.03738.X
- Prokakis C, Koletsis E, Dedeilias P. Airway trauma: a review on epidemiology, mechanisms of injury, diagnosis and treatment. J Cardiothorac Surg. 2014;9. doi:https://doi.org/10.1186/1749-8090-9-117
- Santiago-Rosado L, Sigmon D, Lewison C. Tracheal Trauma. StatPearls Publishing; 2024.
- Capasso R, Carbone M, Rossi E. A 4-year-old child presenting morning onset of spontaneous tracheal rupture due to bronchial mucous plug occlusion during the nighttime sleep: a case report. J Med Case Rep. 2016;10. doi:https://doi.org/10.1186/s13256-016-0912-9
- Piper L, Nam J, Kuckelman J. A case report of combat blast injury requiring combat casualty care, far-forward ECMO, air transport, and all levels of military critical care. Mil Med. 2023;188:1344-1349. doi:https://doi.org/10.1093/milmed/usab354
- Mikheev A, Trushin S. A clinical case of successful treatment of complete abruption of the trachea from the larynx. IP Pavlov Russian Medical Biological Herald. 2021;29:117-124. doi:https://doi.org/10.23888/PAVLOVJ2021291117-124
- Dam V, Mohamad S, Hassan N. A missed diagnosis of laryngotracheal injury secondary to emergency intubation: lessons learned. Acta Med. 2022;65:112-117. doi:https://doi.org/10.14712/18059694.2022.27
- Hone S, Keogh I, Prasad V. A pin in the neck. Ir Med J. 2001;94.
- Shimamoto Y, Sanuki M, Kurita S. A novel case report of iatrogenic tracheal rupture caused by a laser-resistant endotracheal tube under transoral laser laryngeal and nasopharyngeal surgery. Am J Case Rep. 2022;23. doi:https://doi.org/10.12659/AJCR.938357
- Kulkarni M, Prabhu M, Maddineni S. A novel method of airway management in a case of penetrating neck injury. Indian J Anaesth. 2016;60. doi:https://doi.org/10.4103/0019-5049.186019
- Blanc F, Najaf Y, Garrel R. A posttraumatic cervical hematoma with emphysema. J Trauma Acute Care Surg. 2018;85:823-824. doi:https://doi.org/10.1097/TA.0000000000002026
- Erikci V, Hosgör M. A rare complication of the Sistrunk’s procedure in thyroglossal duct remnant: tracheal injury. Ann Pediatr Surg. 2014;10:130-132. doi:https://doi.org/10.1097/01.XPS.0000452065.08719.3c
- Jesani S, Elkattawy S, Ayad S. A rare yet morbid complication of endotracheal intubation: tracheal rupture. Eur J Case Rep Intern Med. 2021;8. doi:https://doi.org/10.12890/2021_002722
- Abu Bakar A. A short cut to definitive airway in open tracheal injury: a case report. Med Health. 2017;12:348-351. doi:https://doi.org/10.17576/MH.2017.1202.20
- Chu J, Sun J, Sheng C. A woman with neck swelling and dyspnea. Ann Emerg Med. 2023;82:E197-E198. doi:https://doi.org/10.1016/j.annemergmed.2023.06.013
- Reihani H, Mahmoudi V, Abbasi B. A young woman with puffy face. J Emerg Med. 2016;51:E97-E99. doi:https://doi.org/10.1016/j.jemermed.2016.05.051
- Grisel J, Richter G, Casper K. Acquired tracheoesophageal fistula following disc-battery ingestion: can we watch and wait?. Int J Pediatr Otorhinolaryngol. 2008;72:699-706. doi:https://doi.org/10.1016/j.ijporl.2008.01.015
- Abughararah T, Adeen A, Althagafi Z. Acquired tracheoesophageal fistula repaired with one-stage surgery without tracheal resection using lateral cervical approach, a case report. Int J Surg Case Rep. 2024;119. doi:https://doi.org/10.1016/j.ijscr.2024.109591
- Oliveira J, Maia N, Gonçalves J. Airway management for penetrating neck trauma: a case report. Cureus. 2023;15. doi:https://doi.org/10.7759/cureus.33441
- Mohammed S, Biyani G, Bhatia P. Airway management in a patient with blunt trauma neck: a concern for anesthesiologist. Egypt J Anaesth. 2014;30:431-433. doi:https://doi.org/10.1016/j.egja.2014.04.002
- Johnson A, Hill J, Zagorski D. Airway management in a patient with tracheal disruption due to penetrating neck trauma with hollow point ammunition: a case report. A A Pract. 2018;10:242-245. doi:https://doi.org/10.1213/XAA.0000000000000675
- Chatterjee D, Agarwal R, Bajaj L. Airway management in laryngotracheal injuries from blunt neck trauma in children. Paediatr Anaesth. 2016;26:132-138. doi:https://doi.org/10.1111/pan.12791
- Sivachalam S, Rajan S, Paul J. Airway management of a patient with laryngotracheal disruption following blunt neck trauma. J Anaesthesiol Clin Pharmacol. 2021;37. doi:https://doi.org/10.4103/JOACP.JOACP_368_18
- Koltka K, Sungur Z, İlhan M. Airway management of major blunt tracheal and esophageal injury: a case report. Ulusal Travma ve Acil Cerrahi Dergisi. 2022;28:120-123. doi:https://doi.org/10.14744/tjtes.2020.81613
- Aribas O, Kanat F, Emlik D. An epidural emphysema due to the tracheal laceration that occurred after a blunt trauma: an extremely rare condition. Eur J Cardiothorac Surg. 2003;24. doi:https://doi.org/10.1016/S1010-7940(03)00395-6
- Sabetian G, Shakibafard A, Borazjani R. An overinflated, normal pressure endotracheal tube cuff sealed a tracheal defect in an 18-year-old man with blunt neck and chest trauma. J Trauma Acute Care Surg. 2021;90:E171-E173. doi:https://doi.org/10.1097/TA.0000000000003181
- Conzo G, Fiorelli A, Palazzo A. An unpredicted case of tracheal necrosis following thyroidectomy. Ann Ital Chir. 2012;83:55-58.
- Singh S, Shilpi A, Sabarigirish K. An unusual case of penetrating neck injury. Nat J Otorhinolaryngol Head Neck Surg. 2013;1:19-20.
- Venkatachalam S, Selvaraj D, Rangarajan M. An unusual case of penetrating tracheal (“cut throat”) injury due to chain snatching: the ideal airway management. Indian J Crit Care Med. 2007;11:151-154. doi:https://doi.org/10.4103/0972-5229.35359
- Yousuf M, Pervez M, Fatimi S. Anaesthetic management of tracheal injury following blunt neck trauma: an unusual late presentation. J Coll Physicians Surg Pak. 2021;31:992-994. doi:https://doi.org/10.29271/jcpsp.2021.08.992
- Heyes R, Cervantes S, Matthaeus J. Balloon dilation causing tracheal rupture: endoscopic management and literature review. Laryngoscope. 2016;126:2774-2777. doi:https://doi.org/10.1002/lary.25977
- Bassi M, Anile M, Pecoraro Y. Bedside transcervical-transtracheal postintubation injury repair in a COVID-19 patient. Ann Thorac Surg. 2020;110:E417-E419. doi:https://doi.org/10.1016/j.athoracsur.2020.04.009
- Kamal Y, Orieby A. Blunt complete tracheal transection. Indian J Surg. 2019;81:89-90. doi:https://doi.org/10.1007/s12262-018-1816-2
- Mukherjee K, Isbell J, Yang E. Blunt posterior tracheal laceration and esophageal injury in a child. J Pediatr Surg. 2009;44:1292-1294. doi:https://doi.org/10.1016/j.jpedsurg.2009.01.012
- Johansson K, Ananda N, Campbell P. Blunt tracheo-oesophageal transsection. Eur J Surg. 2001;167:795-797. doi:https://doi.org/10.1080/11024150152707815
- Li F, Song Y, Wang P. Bronchoscopic intervention for cervical tracheal laceration: a case report and review of the literature. Int J Exp Med. 2020;13:4451-4455.
- Hussein E, Pathak V, Shepherd R. Bronchoscopic management of iatrogenic tracheal laceration using polyurethane-covered nitinol tracheal stents. J Trauma Acute Care Surg. 2016;81:979-983. doi:https://doi.org/10.1097/TA.0000000000001233
- O’Connor A, Cooper J. Case of the month: complete transection of the trachea and oesophagus in a 10 year old child: a difficult airway problem. Emerg Med J. 2006;23:156-159. doi:https://doi.org/10.1136/emj.2004.022368
- Navarro R, Pedraza A, Quach P. Cervical pneumatocele: a case report and review of the literature. Radiol Case Rep. 2024;19:3979-3981. doi:https://doi.org/10.1016/j.radcr.2024.06.030
- Seims A, Shellenberger T, Parrish G. Cervical tracheal transection after scarf entanglement in a go-kart engine. J Emerg Med. 2013;45:E13-E16. doi:https://doi.org/10.1016/j.jemermed.2012.11.072
- Al-Balawi M, Al-Mobaireek K, Alotaibi W. Clinical presentation of air leak in an infant with undiagnosed cystic fibrosis: a case report. J Med Case Rep. 2015;9. doi:https://doi.org/10.1186/s13256-015-0620-x
- Ebrahimian R, Moayerifar M, Gholipour M. Combined tracheoesophageal transection following a life-threatening clothesline-type blunt neck trauma: a case report. Int J Surg Case Rep. 2024;114. doi:https://doi.org/10.1016/j.ijscr.2023.109173
- Feat S, Le Clech G, Riffaud L. Complete cervical tracheal rupture in children after closed trauma. J Pediatr Surg. 2002;37. doi:https://doi.org/10.1053/jpsu.2002.36212
- Paik J, Choi J, Han S. Complete cervical tracheal transection caused by blunt neck trauma: case report. Ulus Travma Acil Cerrahi Derg. 2014;20:459-462. doi:https://doi.org/10.5505/TJTES.2014.32744
- Nitta K, Hamano Y, Kamijo H. Complete cervical tracheal transection due to blunt trauma. Acute Med Surg. 2016;3. doi:https://doi.org/10.1002/AMS2.184
- Norwood S, McAuley C, Vallina V. Complete cervical tracheal transection from blunt trauma. J Trauma. 2001;51:568-571. doi:https://doi.org/10.1097/00005373-200109000-00026
- Ershadi R, Hajipour A, Vakili M. Complete cricotracheal transection due to blunt neck trauma without significant symptoms. J Surg Case Rep. 2017;2017. doi:https://doi.org/10.1093/jscr/rjx111
- Huang H, Ning C, Huo Q. Complete disruption of cervical trachea and esophagus after open injury: a case report and literature review. Int J Clin Exp Med. 2018;11:13920-13924.
- Alharbi S, Najmi A, Alzahrani M. Complete laryngotracheal separation secondary to blunt trauma: a case report. Ear Nose Throat J. 2022;104:158-161. doi:https://doi.org/10.1177/01455613221102869
- Ampollini L, Stavroulias D, Bilancia R. Complete tracheal disruption by motor-saw. Asian Cardiovasc Thorac Ann. 2010;18:399-400. doi:https://doi.org/10.1177/0218492310375623
- Morrison R, Madan A, Raafat A. Complete tracheal disruption following blunt trauma. Eur J Trauma. 2004;30:330-333. doi:https://doi.org/10.1007/s00068-004-1371-3
- Rodríguez Gómez C, Rubio Garay M, Baldó Padró X. Complete tracheal resection in closed cervical spine injury. Arch Broncopneumol. 2016;52. doi:https://doi.org/10.1016/J.ARBR.2016.01.022
- Smith C, Alex G, Zayas-Bazan F. Complete tracheal transection in a 3-year-old after blunt neck trauma: a case report. Rom J Anaesth Intensive Care. 2020;27:4-10. doi:https://doi.org/10.2478/rjaic-2020-0003
- Viswanathan A, Rao M, Palaniappan M. Complete transection of cervical trachea following blunt trauma – A case report. Indian J Thorac Cardiovasc Surg. 2001;17:241-242. doi:https://doi.org/10.1007/s12055-001-0024-y
- Smith D, Rasmussen S, Peng A. Complete traumatic laryngotracheal disruption – A case report and review. Int J Pediatr Otorhinolaryngol. 2009;73:1817-1820. doi:https://doi.org/10.1016/j.ijporl.2009.08.022
- Khan M, Ahmed S, Shakeel M. Complication following primary repair of a penetrating bull horn injury to the trachea. J Emerg Trauma Shock. 2008;1. doi:https://doi.org/10.4103/0974-2700.43199
- Duarte C, Vieira E, Almeida S. Conservative approach of a paediatric tracheal rupture. BMJ Case Rep. 2023;16. doi:https://doi.org/10.1136/bcr-2022-254494
- Mullan G, Georgalas C, Arora A. Conservative management of a major post-intubation tracheal injury and review of current management. Eur Arch Otorhinolaryngol. 2007;264:685-688. doi:https://doi.org/10.1007/s00405-006-0234-4
- Song Z, Jiang Y, Tan J. Conservative management of a rare case of post thyroidectomy tracheal injury with coagulation abnormalities. Heliyon. 2024;10. doi:https://doi.org/10.1016/j.heliyon.2024.e28737
- Materazzi G, Fregoli L, Ribechini A. Conservative management of a tracheal leakage occurring 40 days after robotic thyroidectomy. Otolaryngol Head Neck Surg. 2013;149:793-794. doi:https://doi.org/10.1177/0194599813501781
- Kucuk G, Ates U, Gollu G. Conservative management of tracheal rupture in a child after blunt trauma. Arch Argent Pediatr. 2016;114:E454-E456. doi:https://doi.org/10.5546/aap.2016.eng.e454
- Takahashi T, Kaneko T, Hane A. Conservative medical management combined with follow-up multidetector computed tomography of tracheobronchial injury caused by penetrating injuries: a case report. Trauma Case Rep. 2022;42. doi:https://doi.org/10.1016/j.tcr.2022.100710
- Zuluaga-Gómez M, González-Arroyave D, Ardila C. Conservative medical management of a tracheal perforation after blunt trauma in a patient with SARS-CoV-2. Case Rep Med. 2022;2022. doi:https://doi.org/10.1155/2022/7344476
- Davies G, Leighton S, Hayward R. Jet-ski injury: severe blunt neck trauma with survival. J R Soc Med. 2001;94:402-403. doi:https://doi.org/10.1177/014107680109400808
- Rieth A, Varga E, Kovács T. Contemporary management strategies of blunt tracheobronchial injuries. Injury. 2021;52:S7-S14. doi:https://doi.org/10.1016/j.injury.2020.07.026
- Harjai M, Ramalingam W, Chitkara G. Corrosive tracheo-esophageal fistula following button battery ingestion. Indian Pediatr. 2012;49:145-146.
- Devaraja K, Nayak D, Kamath P. Cough induced pneumomediastinum due to tracheal tear. J Clin Diagn Res. 2018;12:6-8. doi:https://doi.org/10.7860/JCDR/2018/38136.12299
- Vivero R, Saint-Hilaire R, Bhatia R. Cricotracheal separation after gunshot to the neck: report of a survivor with recovery of bilateral vocal fold function. J Emer Med. 2014;46:E27-E30. doi:https://doi.org/10.1016/j.jemermed.2013.08.090
- Malliari H, Ntasenos E, Chatziavramidis A. Cricotracheal separation with multiple cricoid fractures after blunt neck injury: a case report. Hippokratia. 2014;18:65-66.
- Nur Hashima A, Marina M, Sani M. Cricotracheal separation: a case of delayed diagnosis and treatment. Med J Malaysia. 2011;66:144-145.
- McCrystal D, Bond C. Cricotracheal separation: a review and a case with bilateral recovery of recurrent laryngeal nerve function. J Laryngol Otol. 2006;120:497-501. doi:https://doi.org/10.1017/S0022215106000909
- Mevik K, Tysvær G, Solli T. Delayed cervical emphysema after thyroidectomy: a case report and a literature overview. J Surg Case Rep. 2024;2024. doi:https://doi.org/10.1093/jscr/rjae435
- Hsiao S, Chen B, Lee T. Delayed diagnosis of complete tracheal transection after blunt neck trauma. Tzu Chi Med J. 2009;21:77-80. doi:https://doi.org/10.1016/S1016-3190(09)60013-6
- Shew M, Boyd C, Kraft S. Delayed multifocal tracheal injury following thyroidectomy: a case report and review of the literature. Cureus. 2020;12. doi:https://doi.org/10.7759/CUREUS.8164
- Teo L, Chan H, Chiu M. Delayed presentation of an isolated tracheal injury following direct blunt anterior neck trauma. Injury Extra. 2008;39:329-331. doi:https://doi.org/10.1016/j.injury.2008.05.005
- Devaraja K, Kumar R, Sagar P. Delayed presentation of tracheal injury after thyroidectomy – A case report. Indian J Surg. 2018;80:530-532. doi:https://doi.org/10.1007/s12262-018-1748-x
- Azar S, Patel E, Evans L. Delayed tracheal perforation after partial thyroidectomy: a case report and review of the literature. Ear Nose Throat J. 2023;102:NP410-NP412. doi:https://doi.org/10.1177/01455613211019785
- Heo D, Son H, John Sung H. Delayed tracheal perforation after thyroidectomy: a case report and literature review. Ear Nose Throat J. 2025;104:68S-73S. doi:https://doi.org/10.1177/01455613231172888
- Stevens M, Bolduan A, Gelbard A. Delayed tracheal perforation following total thyroidectomy. Laryngoscope. 2022;132:17-19. doi:https://doi.org/10.1002/LARY.29534
- Alevizos L, Tsamis D, Koutsoumanis K. Delayed tracheal rupture after thyroidectomy. Am Surg. 2012;78:E227-E228. doi:https://doi.org/10.1177/000313481207800416
- Damrose E, Damrose J. Delayed tracheal rupture following thyroidectomy. Auris Nasus Larynx. 2009;36:113-115. doi:https://doi.org/10.1016/j.anl.2008.03.007
- Weng Y, Hu B, Jiang J. Delayed tracheal rupture following transoral endoscopic thyroidectomy vestibular approach: case report and review of the literature. Head Neck. 2022;44:E38-E44. doi:https://doi.org/10.1002/HED.27180
- Fette A, Aufdenblatten C, Lang F. Emergency call: trachea rupture in a child. Int J Pediatr Otorhinolaryngol Extra. 2008;3:94-99. doi:https://doi.org/10.1016/j.pedex.2007.12.003
- Varghese K, Sharma P, Sahu S. Emergency lifesaving management of a homicidal cut-throat injury: a case report. Cureus. 2023;15. doi:https://doi.org/10.7759/cureus.47789
- Kiliçgün A, Gezer S, Korkmaz T. Emergent treatment of epidural pneumatosis and pneumomediastinum developed due to tracheal injury: a case report. Turkish J Emerg Med. 2010;10:188-190.
- Han C, Kim E, Lee J. Endotracheal suture through extending tracheostoma for post-tracheostomy tracheal laceration: a case report. J Med Case Rep. 2023;17. doi:https://doi.org/10.1186/S13256-023-03845-W
- Kuo Y, Levine M. Erosion of anterior cervical plate into pharynx with pharyngotracheal fistula. Dysphagia. 2010;25:334-337. doi:https://doi.org/10.1007/s00455-009-9271-7
- Kolleri J, Al-Warqi A, Mohamed R. Extensive surgical emphysema following stab injury to the neck. Cureus. 2021;13. doi:https://doi.org/10.7759/cureus.20126
- Dalal S, Karwasra R, Parshad S. Extensive tracheal injury in penetrating neck trauma – A case report and management discussion. Eur Surg. 2010;42:237-240. doi:https://doi.org/10.1007/s10353-010-0560-z
- Clark J, Morrison J, O’Connor J. Extracorporeal membrane oxygenation support during repair of a noniatrogenic tracheal injury. Ann Thorac Surg. 2022;113:E49-E51. doi:https://doi.org/10.1016/j.athoracsur.2021.03.029
- Mezhir J, Glynn L, Liu D. Handlebar injuries in children: should we raise the bar of suspicion?. Am Surg. 2007;73:807-810.
- Vega C, Patel N, Gonik N. Hypoxic respiratory failure in an adolescent after blunt neck trauma. J Paediatr Child Health. 2021;57:1681-1682. doi:https://doi.org/10.1111/JPC.15327
- Sawhney C, Arora M, Kumar S. Initial management in blunt trauma neck. J Anaesthesiol Clin Pharmacol. 2018;34:275-276. doi:https://doi.org/10.4103/0970-9185.168264
- Joshi M, Mardakh S, Yarmush J. Intraoperatively diagnosed tracheal tear after using an NIM EMG ETT with previously undiagnosed tracheomalacia. Case Rep Anesthesiol. 2013;2013:1-3. doi:https://doi.org/10.1155/2013/568373
- Narci H, Gündüz K, Yandi M. Isolated tracheal rupture caused by blunt trauma and the importance of early diagnosis: a case report. Eur J Emerg Med. 2004;11:217-219. doi:https://doi.org/10.1097/01.mej.0000114646.63700.ef
- Sanna S, Monteverde M, Taurchini M. It could suddenly happen: delayed rupture of the trachea after total thyroidectomy. A case report. G Chir. 2014;35. doi:https://doi.org/10.11138/gchir/2014.35.3.065
- Bertolaccini L, Lauro C, Priotto R. It sometimes happens: late tracheal rupture after total thyroidectomy. Interact Cardiovasc Thorac Surg. 2012;14:500-501. doi:https://doi.org/10.1093/icvts/ivr126
- Paul D, Alhamarneh O, Campbell J. Conservative treatment of delayed tracheal perforation following thyroidectomy. The Otorhinolaryngologist. 2013;6:119-121.
- Baptista De Rezende Neto J, Costa Ferreira G, Da Silva Filho A. Kiting injuries: report of two cases and discussion. J Trauma. 2000;48:310-311. doi:https://doi.org/10.1097/00005373-200002000-00019
- Aouad R, Moutran H, Rassi S. Laryngotracheal disruption after blunt neck trauma. Am J Emerg Med. 2007;25:1084.E1-1084.E2. doi:https://doi.org/10.1016/j.ajem.2007.02.048
- Ajmal M, Najeeb T. Laryngotracheal reconstruction in total laryngotracheal transection. J Coll Physicians Surg Pak. 2008;18:113-114.
- Biswas A, Ahmed F, Milki F. Laryngotracheal separation following blunt neck injury. BJO. 2016;22:114-118. doi:https://doi.org/10.3329/bjo.v22i2.45101
- Humenansky K, Harris T, Hoffman D. Laryngotracheal separation following blunt neck trauma. Am J Emerg Med. 2017;35:669.E5-669.E7. doi:https://doi.org/10.1016/j.ajem.2016.11.031
- Tebala G, Ciani R, Fonsi G. Laryngotracheal trauma: up-to-date report of two cases of a challenging problem. Eur J Trauma. 2006;32:295-299. doi:https://doi.org/10.1007/s00068-006-6013-5
- Thaware P, Trivedi S, Lakra A. Life-saving multidisciplinary management of self-inflicted tracheal transection: a case report. Cureus. 2024;16. doi:https://doi.org/10.7759/cureus.65174
- Stupnik T, Steblaj S, Sok M. Major tracheal tear and bilateral tension pneumothorax complicating percutaneous tracheostomy. Arch Otolaryngol Head Neck Surg. 2009;135:821-823. doi:https://doi.org/10.1001/archoto.2009.88
- Huei T, Lip H, Ranmat O. Major tracheobronchial injuries: management of two rare cases. Med J Malaysia. 2018;73:177-179.
- Barrett E. Management of a traumatic tracheal tear: a case report. AANA J. 2011;79:468-470.
- O’Callaghan J, Keh S, D’Souza A. Management of closed tracheal perforation following blunt trauma. Otolaryngol Head Neck Surg. 2009;141:661-662. doi:https://doi.org/10.1016/j.otohns.2009.05.007
- Debs S, Petersson R, Wong S. Management of dog-related penetrating laryngotracheal trauma in a pediatric patient. Cureus. 2023;15. doi:https://doi.org/10.7759/cureus.48470
- Shibahashi K, Numata K. Nail gun injury of the trachea and spinal cord. Clin Pract Cases Emerg Med. 2022;6:252-253. doi:https://doi.org/10.5811/cpcem.2022.3.56410
- Schellenberg M, Inaba K, Warriner Z. Near hangings: epidemiology, injuries, and investigations. J Trauma Acute Care Surg. 2019;86:454-457. doi:https://doi.org/10.1097/TA.0000000000002134
- Verettas D, Karapantsos E, Boyatzis C. Neglected hangman’s fracture in association with rupture of the trachea. Spine J. 2008;8:552-554. doi:https://doi.org/10.1016/j.spinee.2007.01.007
- Huber K, Billington A, Taylor L. Nonoperative treatment of a tracheocutaneous fistula in a burn patient. J Burn Care Res. 2017;38:E772-E775. doi:https://doi.org/10.1097/BCR.0000000000000473
- Loroch A, Curran J, Wynne D. Paediatric longitudinal tracheal laceration from blunt force trauma: a case report. Cureus. 2021;13. doi:https://doi.org/10.7759/cureus.19867
- Nicholson B, Dhindsa H, Seay L. Pediatric blunt neck trauma causing esophageal and complete tracheal transection. Prehosp Emerg Care. 2017;21:257-262. doi:https://doi.org/10.1080/10903127.2016.1229822
- Jitpakdee P, Steele T, Bhuskute A. Pediatric laryngotracheal separation following a go-cart injury. Int J Pediatr Otorhinolaryngol. 2016;85:166-169. doi:https://doi.org/10.1016/j.ijporl.2016.03.030
- Marathe U, Tran L. Pediatric neck trauma causing massive subcutaneous emphysema. J Trauma. 2006;61:440-443. doi:https://doi.org/10.1097/01.TA.0000229909.39338.CE
- Kho J, Ong E, Tang I. Penetrating neck injury: selective surgery versus urgent exploration?. Acta Otolaryngol Case Rep. 2016;1:106-109. doi:https://doi.org/10.1080/23772484.2016.1248230
- Archan S, Gumpert R. Penetrating neck trauma causing tracheal rupture, spinal cord injury, and massive pneumocephalus. Am J Emerg Med. 2010;28:254.E1-254.E2. doi:https://doi.org/10.1016/j.ajem.2009.05.004
- Al Harakeh H, Tulimat T, Sfeir P. Penetrating shrapnel injury to the chest presenting as a delayed tracheoesophageal fistula (TEF). A case report. Trauma Case Rep. 2018;17:5-8. doi:https://doi.org/10.1016/j.tcr.2018.09.002
- Akaraviputh T, Angkurawaranon C, Phanchaipetch T. Platysma myocutaneous flap interposition in surgical management of large acquired post-traumatic tracheoesophageal fistula: a case report. Int J Surg Case Rep. 2014;5:282-286. doi:https://doi.org/10.1016/j.ijscr.2014.03.017
- Turgut K, Algın A, Apaydın H. Pneumomediastinum due to penetrating neck injury: a case report. Istanbul Med J. 2019;20:267-269. doi:https://doi.org/10.4274/imj.galenos.2018.82956
- Amore D, Casazza D, Caterino U. Post-intubation tracheoesophageal fistula: surgical management by complete cervical tracheal transection. Ann Thorac Cardiovasc Surg. 2024;30:22-00134. doi:https://doi.org/10.5761/atcs.cr.22-00134
- Salih A, Kakamad F, Habibullah I. Post-thyroidectomy tracheocutaneous fistula; a case report with literature review. Int J Surg Case Rep. 2020;72:172-174. doi:https://doi.org/10.1016/j.ijscr.2020.05.055
- Chaaban S, Simoff M, Ray C. Posterior tracheal laceration treated with a stent. Ann Am Thorac Soc. 2017;14:1224-1226. doi:https://doi.org/10.1513/AnnalsATS.201611-937CC
- Claes I, Van Schil P, Corthouts B. Posterior tracheal wall laceration after blunt neck trauma in children: a case report and review of the literature. Resuscitation. 2004;63:97-102. doi:https://doi.org/10.1016/j.resuscitation.2004.04.016
- Kutlu R, Kuzucu A, Soysal Ö. Postintubation tracheal rupture. Asian Cardiovasc Thorac Ann. 2001;150:150-152.
- MacDougall P. Postoperative tracheal rupture in a patient with a difficult airway. Canadian J Anesth. 2006;53:385-388. doi:https://doi.org/10.1007/BF03022504
- Pongsapich W, Chongkolwatana C, Ratanaprasert N. Prawn rostrum, a rare migratory esophageal foreign body penetrating the trachea. Otolaryngol Case Reports. 2020;15. doi:https://doi.org/10.1016/j.xocr.2020.100172
- Linnau K, Cohen W, Mann F. Radiologic evaluation of attempted suicide by hanging: cricotracheal separation and common carotid artery dissection. AJR Am J Roentgenol. 2002;178. doi:https://doi.org/10.2214/AJR.178.1.1780214
- Parage F, Vashisht A, Sisodia V. Reconstruction of complete tracheal transection with cardiopulmonary bypass support following bull horn injury in neck during coronavirus disease 19 pandemic lockdown. Indian J Thorac Cardiovasc Surg. 2021;37:442-446. doi:https://doi.org/10.1007/s12055-020-01098-6
- Gopal M, Westgarth-Taylor C, Loveland J. Repair of tracheo-oesophageal fistula secondary to button battery ingestion: a combined cervical and median sternotomy approach. Afr J Paediatr Surg. 2015;12:91-93. doi:https://doi.org/10.4103/0189-6725.151003
- O’Connor J, Haan J, Wright J. Spent bullet in the bronchus. Am Surg. 2006;72:345-346. doi:https://doi.org/10.1177/000313480607200414
- Akhlaq S, Ejaz T, Aziz A. Spontaneous pneumomediastinum in accidental chlorine gas inhalational injury: case report and review of literature. BMJ Case Rep. 2021;14. doi:https://doi.org/10.1136/bcr-2020-236549
- Roh J, Lee J. Spontaneous tracheal rupture after severe coughing in a 7-year-old boy. Pediatrics. 2006;118:E224-E227. doi:https://doi.org/10.1542/peds.2005-3019
- Stevens M, Mullis T, Carron J. Spontaneous tracheal rupture caused by vomiting. Am J Otolaryngol. 2010;31:276-278. doi:https://doi.org/10.1016/j.amjoto.2009.02.008
- Kaneko Y, Nakazawa K, Yokoyama K. Subcutaneous emphysema and pneumomediastinum after translaryngeal intubation: tracheal perforation due to unsuccessful fiberoptic tracheal intubation. J Clin Anesth. 2006;18:135-137. doi:https://doi.org/10.1016/j.jclinane.2005.10.006
- Gupta B, Bagaria D, Kumar A. Successful airway management of traumatic complete tracheal transection. BMJ Case Rep. 2022;15. doi:https://doi.org/10.1136/bcr-2022-251688
- Oh J, Hong S, Kang S. Successful conservative management of tracheal injury after forceful coughing during extubation: a case report. Anesth Pain Med. 2016;6. doi:https://doi.org/10.5812/aapm.39262
- Guillamondegui O, Nance M, Gaynor J. Successful management of concomitant blunt injury to the trachea, esophagus, and cervical spine in a 6-year-old girl. J Pediatr Surg. 2004;39:1130-1132. doi:https://doi.org/10.1016/j.jpedsurg.2004.03.078
- Naqvi Sayyed E, Sadik A, Beg M. Successful management of suicidal cut throat injury with internal jugular, tracheal and esophageal transection: a case report. Trauma Case Rep. 2018;13:30-34. doi:https://doi.org/10.1016/j.tcr.2017.11.005
- Salehuddin N, Saniasiaya J, Hamid S. Successful non-surgical management of extensive tracheal injury. Gazi Medical Journal. 2020;31:680-682. doi:https://doi.org/10.12996/GMJ.2020.158
- Jeong H, Choi K, Oh Y. Suicidal hanging patient with complete tracheal rupture. Hong Kong J Emerg Med. 2019;26:124-126. doi:https://doi.org/10.1177/1024907918762870
- Khanum T, Jawaid M, Zia S. Surgical blowhole incision – An unconventional approach to subcutaneous emphysema management following blunt neck trauma. J Coll Phys Surg Pak. 2022;32:665-667. doi:https://doi.org/10.29271/jcpsp.2022.05.665
- Valerio P, Macia I, Francisco R. Survival after traumatic complete laryngotracheal transection. Am J Emerg Med. 2008;26:837.E3-837.E4. doi:https://doi.org/10.1016/j.ajem.2008.01.031
- Ahmad M, Sinha P, Al-Tamimi Y. The Isadora syndrome: a case report of cervical, oesophageal and tracheal transection in a go-karting accident. Br J Neurosurg. 2011;25:310-312. doi:https://doi.org/10.3109/02688697.2010.544788
- Losken A, Rozycki G, Feliciano D. The use of the sternocleidomastoid muscle flap in combined injuries to the esophagus and carotid artery or trachea. J Trauma. 2000;49:815-817. doi:https://doi.org/10.1097/00005373-200011000-00004
- Dumanlı A, Gencer A, User N. Total cervical tracheal rupture following blunt trauma. Tuberk Toraks. 2018;66:345-348. doi:https://doi.org/10.5578/tt.67717
- Blanc F, Blanchet C, Mondain M. Tracheal injury complicating Sistrunk’s thyroglossal cyst surgery. Eur Ann Otorhinolaryngol Head Neck Dis. 2020;137:131-133. doi:https://doi.org/10.1016/j.anorl.2019.10.005
- George S, Samarasam I, Mathew G. Surgical gastroenterology tracheal injury during oesophagectomy-incidence, treatment and outcome. Trop Gastroenterol. 2011;32:309-313.
- Miyawaki M, Ogawa K, Kamada K. Tracheal injury from dog bite in a child. J Cardiothorac Surg. 2023;18. doi:https://doi.org/10.1186/s13019-023-02107-6
- Motloung E, Mapholi S, As A. Tracheal injury in a toddler. S Afr Med J. 2021;111:1142-1144. doi:https://doi.org/10.7196/SAMJ.2021.v111i11b.16100
- Park H, Lee S, Shin H. Tracheal laceration detected by high end-tidal CO2 during endoscopic thyroidectomy. Korean J Anesthesiol. 2009;56. doi:https://doi.org/10.4097/kjae.2009.56.6.703
- Chen K, Lee S, Ko T. Tracheal ring fracture as a consequence of external laryngeal manipulation during endotracheal intubation. Acta Anaesthesiol Taiwan. 2009;47:103-105. doi:https://doi.org/10.1016/S1875-4597(09)60034-5
- Raskin J, Borrelli M, Nasrollahi T. Tracheal rupture after tracheostomy tube exchange in a patient with recurrent oral cavity spindle cell carcinoma. Ear Nose Throat J. 2022;101:15S-18S. doi:https://doi.org/10.1177/01455613221123854
- Akkas M, Tiambeng C, Aksu N. Tracheal rupture as a result of coughing. Am J Emerg Med. 2018;36:2133.E1-2133.E3. doi:https://doi.org/10.1016/j.ajem.2018.08.027
- Eipe N, Choudhrie A. Tracheal rupture in a child with blunt chest injury. Paediatr Anaesth. 2007;17:273-277. doi:https://doi.org/10.1111/j.1460-9592.2006.02076.x
- Mener D, Stewart F, Tunkel D. Tracheal tear from blunt neck trauma in children: diagnosis and management. Int J Pediatr Otorhinolaryngol. 2017;96:100-102. doi:https://doi.org/10.1016/j.ijporl.2017.03.010
- Hsueh W, Wang S, Liu T. Tracheal transection caused by clothesline injury. J Formos Med Assoc. 2014;113:573-574. doi:https://doi.org/10.1016/j.jfma.2012.06.004
- Dayal S, Dugom P, Kharazi A. Tracheal transection from gunshot wound to the neck. Ann Thorac Surg. 2022;114:E39-E41. doi:https://doi.org/10.1016/j.athoracsur.2021.08.076
- Reynolds J, Dart B, Maxwell R. Tracheal transection with associated bilateral carotid and esophageal injuries after blunt neck trauma. Am Surg. 2014;80:E232-E233. doi:https://doi.org/10.1177/000313481408000807
- Sakatoku Y, Fukaya M, Fujieda H. Tracheoesophageal fistula after total resection of gastric conduit for gastro-aortic fistula due to gastric ulcer. Surg Case Rep. 2017;3. doi:https://doi.org/10.1186/s40792-017-0371-6
- Kulyapina A, Díaz D, Rodríguez T. Tracheoinnominate fistula: a rare acute complication of penetrating neck injury. Asian Cardiovasc Thorac Ann. 2015;23:478-480. doi:https://doi.org/10.1177/0218492314540918
- Sezer H, Dayanir H, Zıraman M. Traffic accident like suicide. Eurasian J Pulmonol. 2019;21. doi:https://doi.org/10.4103/ejop.ejop_40_18
- Smith C, Maxson R, Richter G. Trans-cervical tracheal resection and repair of acquired tracheoesophageal fistula secondary to button battery ingestion. J Pediatr Surg Case Rep. 2016;9:11-14. doi:https://doi.org/10.1016/j.epsc.2016.03.017
- Hamid U, McGuigan J, Jones J. Transection of the aerodigestive tract after blunt neck trauma. Ann Thorac Surg. 2011;92:1896-1898. doi:https://doi.org/10.1016/j.athoracsur.2011.04.085
- Fernández E, Moreno Luna R, Navas F. Transverse cervicothoracic stabbing: multidisciplinary management of a surgical emergency. Turk Arch Otolaryngol. 2017;55:144-147. doi:https://doi.org/10.5152/tao.2017.2273
- Nadour K, Hemmaoui B, En-Nafaa I. Traumatic tracheal injury in a child. Eur Ann Otorhinolaryngol Head Neck Dis. 2016;133:223-224. doi:https://doi.org/10.1016/j.anorl.2015.08.029
- Markus-Rodden M, Bojko T, Hauck L. Traumatic tracheal laceration in a pediatric patient medically managed with high-frequency oscillatory ventilation. Pediatr Emerg Care. 2008;24:236-237. doi:https://doi.org/10.1097/PEC.0b013e31816b7b70
- Barasa J, Nthumba P, Bird P. Traumatic tracheostomy and spent bullet aspiration after a gunshot injury: a case report. Ear Nose Throat J. 2013;92. doi:https://doi.org/10.1177/014556131309200820
- Ozpolat B, Atinkaya C, Ozdemir N. Treatment of iatrogenic tracheal laceration with cervical mediastinotomy and tube drainage; a case report. JCAM. 2011;2:55-56. doi:https://doi.org/10.4328/JCAM.24
- Winegarner A, Lecamwasam H, Kendall M. Two endotracheal tubes in one trachea with a traumatic injury. Case Rep Anesthesiol. 2021;2021. doi:https://doi.org/10.1155/2021/9912553
- Shimizu J, Hirano Y, Ishida Y. Use of a silicone T-tube for management of a tracheal injury in a patient with cervical blunt trauma. Jpn J Thorac Cardiovasc Surg. 2003;51:541-544. doi:https://doi.org/10.1007/S11748-003-0120-6
- Lee D, Yoon T, Lee J. Vocal cord paralysis and tracheal rupture secondary to thyroid abscess. Surg Pract. 2016;20:49-51. doi:https://doi.org/10.1111/1744-1633.12164
- Farley L, Schlicksup K. Tracheal injury. Trauma (United Kingdom). 2023;18:155-158. doi:https://doi.org/10.1177/1460408615594389
- Lee W, Eliashar R, Eliachar I. Acute external laryngotracheal trauma: diagnosis and management. Ear Nose Throat J. 2006;85.
- Nahum A, Siegel A. Biodynamics of injury to the larynx in automobile collisions. Ann Otol Rhinol Laryngol. 1967;76:781-785. doi:https://doi.org/10.1177/000348946707600406
- Harris R, Joseph A. Acute tracheal rupture related to endotracheal intubation: case report. J Emerg Med. 2000;18:35-39. doi:https://doi.org/10.1016/S0736-4679(99)00159-6
- Duval E, Geraerts S, Brackel H. Management of blunt tracheal trauma in children: a case series and review of the literature. Eur J Pediatr. 2007;166:559-563. doi:https://doi.org/10.1007/s00431-006-0279-9
- Sippel M, Putensen C, Hirner A. Tracheal rupture after endotracheal intubation: experience with management in 13 cases. Thorac Cardiovasc Surg. 2006;54:51-56. doi:https://doi.org/10.1055/s-2005-865917
- Wood J, Thornton B, Brown C. Traumatic tracheal injury in children: a case series supporting conservative management. Int J Pediatr Otorhinolaryngol. 2015;79:716-720. doi:https://doi.org/10.1016/j.ijporl.2015.02.025
- Cardillo G, Carbone L, Carleo F. Tracheal lacerations after endotracheal intubation: a proposed morphological classification to guide non-surgical treatment. Eur J Cardiothorac Surg. 2009;37:581-587. doi:https://doi.org/10.1016/j.ejcts.2009.07.034
- Han X, Mu Q, Liu C. Covered stent implantation in the treatment of tracheal rupture after thyroidectomy. J Vasc Interv Radiol. 2016;27:1758-1761. doi:https://doi.org/10.1016/j.jvir.2016.04.017
- Da Silva Costa A, Juliano Perfeito J, Succi J. A video-assisted endotracheal suture technique for correction of distal tracheal laceration after intubation. Ann Thorac Surg. 2012;93:2073-2075. doi:https://doi.org/10.1016/j.athoracsur.2011.11.018
- Janni A, Menconi G, Mussi A. Postintubation tracheal tear repair by cervicotomy and longitudinal tracheotomy. Ann Thorac Surg. 2000;69:243-244. doi:https://doi.org/10.1016/S0003-4975(99)01319-3
- Bowley D, Plani F, Murillo D. Intubated, ventilating patients with complete tracheal transection: a diagnostic challenge. Ann R Coll Surg Engl. 2003;85:245-247. doi:https://doi.org/10.1308/003588403766274944
- Lyons J, Feliciano D, Wyrzykowski A. Modern management of penetrating tracheal injuries. Am Surg. 2013;79:188-193.
- Leoncini G, Iurilli L, Boni L. Treatment of iatrogenic and traumatic tracheal disruptions. Monaldi Arch Chest Dis. 2008;69:119-127. doi:https://doi.org/10.4081/monaldi.2008.389
- Herrmann D, Volmerig J, Al-Turki A. Does less surgical trauma result in better outcome in management of iatrogenic tracheobronchial laceration?. J Thorac Dis. 2019;11:4772-4781. doi:https://doi.org/10.21037/jtd.2019.10.22
- Chandra T, Sadhana O, Sameera G. Management of cervical tracheo-esophageal fistula by lateral cervical approach: our experience. Indian J Otolaryngol Head Neck Surg. 2022;74:6039-6044. doi:https://doi.org/10.1007/s12070-021-02682-x
- Kaintura M, Wadhera R, Hernot S. Our 12 year experience with Montgomery T-tube in the management of acute blunt laryngotracheal trauma patients. Braz J Otorhinolaryngol. 2022;88:316-330. doi:https://doi.org/10.1016/j.bjorl.2020.06.009
- Huang C. Use of the silicone T-tube to treat tracheal stenosis or tracheal injury. Ann Thorac Cardiovasc Surg. 2001;7:192-196.
- Liu J, Wu W, Liu S. A modified tracheal transection approach for the repair of nonmalignant tracheoesophageal fistulas: a report of 5 cases. ORL J Otorhinolaryngol Relat Spec. 2017;79:147-152. doi:https://doi.org/10.1159/000468943
- Cassada D, Munyikwa M, Moniz M. Acute injuries of the trachea and major bronchi: importance of early diagnosis. Ann Thorac Surg. 2000;69:1563-1567. doi:https://doi.org/10.1016/s0003-4975(00)01077-8
- Almasi M, Andrasovska M, Koval J. Blunt external trauma to the trachea: report of two cases. B-ENT. 2005;2:93-96.
- Evermann M, Roesner I, Denk-Linnert D. Cervical repair of iatrogenic tracheobronchial injury by tracheal T-incision. Ann Thorac Surg. 2022;114:1863-1870. doi:https://doi.org/10.1016/j.athoracsur.2022.03.019
- Ye D, Shen Z, Zhang Y. Clinical features and management of closed injury of the cervical trachea due to blunt trauma. Scand J Trauma Resusc Emerg Med. 2013;21. doi:https://doi.org/10.1186/1757-7241-21-60
- Wu M, Tsai Y, Lin M. Complete laryngotracheal disruption caused by blunt injury. Ann Thorac Surg. 2004;77:1211-1215. doi:https://doi.org/10.1016/j.athoracsur.2003.08.003
- Cunningham L, Jatana K, Grischkan J. Conservative management of iatrogenic membranous tracheal wall injury: a discussion of 2 successful pediatric cases. JAMA Otolaryngol Head Neck Surg. 2013;139:405-410. doi:https://doi.org/10.1001/jamaoto.2013.75
- Elbadan H, Donia M, Mina A. Cricotracheal separation: do not get fooled by what you see. Eur Arch Otorhinolaryngol. 2021;278:471-476. doi:https://doi.org/10.1007/s00405-020-06140-2
- Bin Pervez M, Mushtaq H, Chauhan S. Delay between onset of indication and definitive surgery for tracheal trauma. J Pak Med Assoc. 2020;70:S110-S112.
- Mubarak Y, Bary M. Experience of emergency cervical tracheal repair after non-iatrogenic injury. Heart Surg Forum. 2021;24:E1-E3. doi:https://doi.org/10.1532/hsf.3349
- Frost A, Ruszkay N, Steinberg T. Iatrogenic tracheal injuries: case series and review of the literature. ORL J Otorhinolaryngol Relat Spec. 2021;83:123-126. doi:https://doi.org/10.1159/000511712
- Yalçin Ş, Ciftci A, Karnak I. Management of acquired tracheoesophageal fistula with various clinical presentations. J Pediatr Surg. 2011;46:1887-1892. doi:https://doi.org/10.1016/j.jpedsurg.2011.06.025
- Li H, Li J, Zhao J. Management of paediatric laryngotracheal trauma. J Laryngol Otol. 2022;136:1125-1129. doi:https://doi.org/10.1017/S0022215121003972
- Carbognani P, Bobbio A, Cattelani L. Management of postintubation membranous tracheal rupture. Ann Thorac Surg. 2004;77:406-409. doi:https://doi.org/10.1016/S0003-4975(03)01344-4
- Hsu W, Schweiger C, Hart C. Management of the disrupted airway in children. Laryngoscope. 2021;131:921-924. doi:https://doi.org/10.1002/LARY.29051
- Guo X, Ji H. Management of tracheal perforation following anterior cervical spine surgery: report of two cases and review of the literature. Case Rep Orthop. 2022;2022:1-7. doi:https://doi.org/10.1155/2022/1914642
- Corsten G, Robert Berkowitz F, Melbourne F. Membranous tracheal rupture in children following minor blunt cervical trauma. Ann Otol Rhinol Laryngol. 2002;3:197-199. doi:https://doi.org/10.1177/000348940211100301
- Aerni M, Parambil J, Allen M. Nontraumatic disruption of the fibrocartilaginous trachea: causes and clinical outcomes. Chest. 2006;130:1143-1149. doi:https://doi.org/10.1378/chest.130.4.1143
- Łochowski M, Kaczmarski J, Brzeziński D. Penetrating neck traumas. Kardiochir Torakochirurgia Pol. 2014;11:30-33. doi:https://doi.org/10.5114/kitp.2014.41927
- Mazita A, Sani A. Sequelae of traumatic laryngotracheal separation: the need for individualized long term treatment plan. Auris Nasus Larynx. 2005;32:421-425. doi:https://doi.org/10.1016/j.anl.2005.05.002
- Gómez-Caro Andrés A, Moradiellos Díez F, Ausín Herrero P. Successful conservative management in iatrogenic tracheobronchial injury. Ann Thorac Surg. 2005;79:1872-1878. doi:https://doi.org/10.1016/j.athoracsur.2004.10.006
- Mahieu H, de Bree R, Ekkelkamp S. Tracheal and laryngeal rupture in neonates: complication of delivery or of intubation?. Ann Otol Rhinol Laryngol. 2004;113:786-792. doi:https://doi.org/10.1177/000348940411301003
- Pan P, Liu T, Li W. Tracheal penetrating injury and airway management: a review of two cases. J Cardiothorac Vasc Anesth. 2024;38:1734-1737. doi:https://doi.org/10.1053/j.jvca.2024.05.017
- Atalay C, Aykan Ş, Can A. Tracheal rupture due to diffusion of nitrous oxide to cuff of high-volume, low-pressure intubation tube. Eurasian J Med. 2009;41:136-139.
- Seidl R, Todt I, Westhofen M. Tracheal rupture in burns-a retrospective study. Burns. 2008;34:525-530. doi:https://doi.org/10.1016/j.burns.2007.06.017
- Borowski D, Mehrotra P, Tennant D. Unusual presentation of blunt laryngeal injury with cricotracheal disruption by attempted hanging: a case report. Am J Otolaryngol. 2004;25:195-198. doi:https://doi.org/10.1016/j.amjoto.2003.11.001
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 522 times
- PDF downloaded - 71 times