Rhinology
Vol. 46: Issue 3 - June 2026
Cross-cultural adaptation of the Italian Chronic Rhinosinusitis Patient-Reported Outcome. Questionnaire
Authors
Antonino Maniaci
 , Luca Giovanni Locatello
, Gian Luca Fadda
, Paolo Boscolo-Rizzo
, Eugenio De Corso
, Jérôme R. Lechien
, Christian Calvo-Henriquez
, Leigh J. Sowerby
, Alberto Maria Saibene
, Luca Giovanni Locatello
, Gian Luca Fadda
, Paolo Boscolo-Rizzo
, Eugenio De Corso
, Jérôme R. Lechien
, Christian Calvo-Henriquez
, Leigh J. Sowerby
, Alberto Maria Saibene
Summary
Cover Image
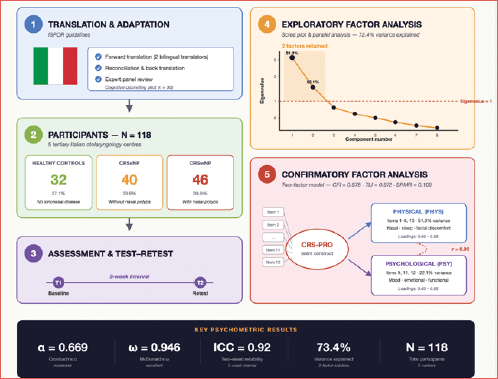
Objective. The Chronic Rhinosinusitis Patient-Reported Outcome (CRS-PRO) is a validated 12- item tool for assessing symptom burden in chronic rhinosinusitis (CRS). Although cross-culturally validated in other languages, there is no Italian version. This study aimed to translate, adapt, and validate the CRS-PRO for Italian-speaking patients.
Methods. We conducted a prospective multicentre study in 5 Italian otolaryngology centres (Jan 2024 - Aug 2025). Translation and adaptation followed International Society for Pharmacoeconomics and Outcomes Research guidelines. Participants were adults with CRS without polyps (CRSsNP), with polyps (CRSwNP), and healthy controls. Psychometric testing included internal consistency (Cronbach’s α, McDonald’s ω), test-retest reliability (Intraclass Correlation Coefficient, ICC), Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) factor analyses, and construct validity.
Results. A total of 118 participants were enrolled (controls = 32, CRSsNP = 40, CRSwNP = 46). Internal consistency was moderate (Cronbach’s α = 0.669) but excellent (McDonald’s ω = 0.946). Reliability was high (ICC = 0.92). EFA supported a two-factor solution (physical, psychological), explaining 73.4% of the total variance. CFA confirmed this model (CFI = 0.978, TLI = 0.972, SRMR = 0.109), with strong interfactor correlation (r = 0.93). CRSwNP patients reported the highest burden.
Conclusions. The Italian CRS-PRO showed strong reliability, validity, and factorial structure, supporting its clinical and research use.
Introduction
Chronic rhinosinusitis (CRS) is a prevalent and heterogeneous inflammatory condition that significantly impacts patients’ quality of life, encompassing physical symptoms, sensory impairments, and psychosocial burden. Although the Sino-Nasal Outcome Test-22 (SNOT-22) is widely used, concerns remain regarding its psychometric limitations and disproportionate weighting of domains such as sleep and emotional dysfunction 1. To overcome these shortcomings, Ghadersohi et al. developed the 12-item Chronic Rhinosinusitis Patient-Reported Outcome (CRS-PRO) instrument using rigorous patient-centred methods. The CRS-PRO demonstrated excellent internal consistency (Cronbach’s α = 0.86), high test–retest reliability (Intraclass Correlation Coefficient, ICC = 0.89), and strong concurrent validity with SNOT-22 (r = 0.83) 2. Subsequent evaluations have supported the CRS-PRO’s responsiveness to clinical changes, including treatment effects measured through objective tools which align with FDA-endorsed PRO development standards 3. Cross-cultural validation studies have extended the CRS-PRO’s utility. The Portuguese adaptation, following International Society for Pharmacoeconomics and Outcomes Research (ISPOR) guidelines, showed good to excellent reliability (ICC 0.65-0.89) across CRSwNP patients 4. Similarly, the Hebrew version demonstrated high internal consistency (Cronbach’s α = 0.936) and discriminative validity between healthy controls and CRS patients, including post-functional endoscopic sinus surgery (FESS) cases 5. Additional validations in languages such as Arabic, French, and Spanish further support the instrument’s global adaptability 6-8. Despite the proliferation of these adaptations, no Italian validation exists to date. To address this gap – crucial for clinical and research applications in Italian-speaking populations – we conducted a prospective, multicentre, observational, cross-cultural validation study to translate, adapt, and assess the psychometric properties of the Italian CRS-PRO (Cover figure).
Materials and methods
Study design and setting
We conducted a prospective, multicentre, observational study aimed at the cross-cultural adaptation and psychometric validation of the Italian version of the CRS-PRO questionnaire. The study was carried out across 5 tertiary otolaryngology centres in Italy between 1 January 2024 and 1 August 2025 (Fig. 1). The protocol was developed and reported according to the Strenghtening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines 9.
Participants
Eligible participants were adults (≥ 18 years) with a confirmed diagnosis of chronic rhinosinusitis without nasal polyps (CRSsNP) or with nasal polyps (CRSwNP), according to EPOS criteria, as well as healthy controls without sinonasal disease. Exclusion criteria included previous major craniofacial surgery, psychiatric disorders interfering with questionnaire completion, or insufficient Italian language proficiency.
Cross-cultural adaptation procedure
The translation and cross-cultural adaptation of the CRS-PRO followed international guidelines, including forward translation by 2 independent bilingual translators, reconciliation, backward translation, and expert panel review. Cognitive debriefing interviews with a pilot sample of patients (n = 30) were conducted to ensure clarity, semantic equivalence, and cultural relevance. The final Italian CRS-PRO was then administered to the study cohort. The full version of the translated Italian version is presented below (Fig. 2).
Data collection
Sociodemographic and clinical data were collected at baseline, including age, gender, smoking status, presence of atopy, asthma comorbidity, previous FESS, and ongoing biologic therapy in CRSwNP patients. Each participant completed the Italian CRS-PRO at enrollment (T1). All patients repeated the CRS-PRO after a 2-week interval (T2) to assess the test–retest reliability.
Statistical analysis
Descriptive statistics were computed for demographic and clinical variables. Internal consistency was evaluated using Cronbach’s α and McDonald’s ω coefficients. Test-retest reliability was assessed through ICC, two-way mixed effects model, absolute agreement. Construct validity was investigated via exploratory factor analysis (EFA) using minimum residual extraction, Oblimin rotation, and parallel analysis on a polychoric correlation matrix. Confirmatory factor analysis (CFA) was subsequently performed using robust DWLS estimation, with model fit assessed by χ2, CFI, TLI, RMSEA (95% CI), and SRMR indices.
The sample size adequacy for factor analysis was calculated according to the psychometric criteria. With 118 respondents and 12 items, our subject-to-item ratio (9.8:1) was well within the recommended range of 5-10 for EFA validity. Furthermore, CFA was estimated using a DWLS approach, which has been demonstrated to generate consistent and stable parameter estimates when applied to small- to moderate samples of models with low complexity. Thus, the number of subjects evaluated was enough to accommodate both factorial analysis and interpretation of model fit indices. Item-scale correlations and floor/ceiling effects were examined to further evaluate the scale’s performance. All analyses were conducted using Jamovi (version 2.6) and R (Version 4.5.1). A significance threshold of p < 0.05 was adopted. Written informed consent was obtained from all participants, and the study was approved by the local institutional ethics committees of the participating centres.
Results
Participant characteristics
A total of 118 participants were enrolled, comprising healthy controls (n = 32), patients with CRSsNP (n = 40), and patients with CRSwNP (n = 46). The sample was evenly distributed by gender (50% male, 50% female). These data are summarised in Table I.
Atopy was present in 36.4% of the participants, and asthma was reported in 30.5%. With respect to smoking status, 60.2% were never-smokers, 28% were former smokers, and 11.9% were current smokers. Prior FESS was reported in 48.3% of cases, exclusively in the CRS subgroups, while 18.6% of CRSwNP patients were receiving biologic therapy at the time of evaluation.
Reliability analysis
Internal consistency of the CRS-PRO was assessed using Cronbach’s α and McDonald’s ω. For the full scale, Cronbach’s α was 0.669, while McDonald’s ω indicated excellent reliability (0.946). Item-level analysis demonstrated that removal of any single item did not significantly improve internal consistency (α ranged 0.611-0.945; ω ranged 0.937-0.949) (Tab. II).
Notably, item 12 (mood disturbance) showed the highest impact on the α coefficient, reflecting its unique psychological contribution relative to the physical symptom cluster.
Exploratory Factor Analysis (EFA)
EFA using minimum residual extraction with Oblimin rotation and parallel analysis on a polychoric correlation matrix suggested a two-factor solution, accounting for 73.4% of total variance (Factor 1: 51.3%; Factor 2: 22.1%) (Tab. III).
The factors corresponded to physical symptoms (items 1-8, 10) and psychological/functional impact (items 9, 11, 12), with moderate correlation (r = 0.374) between them (Fig. 3). Two models were subsequently tested with a robust DWLS estimator. The unidimensional model (Model 1) showed good incremental fit indices (CFI = 0.977; TLI = 0.972; SRMR = 0.111), but an unsatisfactory RMSEA = 0.285 (95% CI [0.264-0.306]) (Tab. IV). The two-factor model (Model 2: PHYS + PSY) yielded similar incremental fit (CFI = 0.978; TLI = 0.972; SRMR = 0.109) with high interfactor correlation (r = 0.93), again suggesting strong overlap between domains while supporting a theoretically meaningful two-factor structure (Fig. 4). The model includes a physical symptoms factor (PHYS; items 1-8, 10) and a psychological factor (PSY; items 9, 11, 12). Standardised factor loadings ranged from 0.65 to 0.99. The correlation between PHYS and PSY was strong (r = 0.93), indicating substantial overlap between domains.
Discussion
This study provides the first cross-cultural adaptation and psychometric validation of the CRS-PRO into Italian. Our findings demonstrate that the Italian CRS-PRO is a reliable and valid instrument for assessing symptom burden in patients with CRS, in line with prior validations in other languages2,4-8.
Internal consistency measures also supported satisfactory reliability of the Italian CRS-PRO, and the item-level analysis demonstrated a good contribution to the scale of all factors 10. Item-level analysis confirmed that all items contributed meaningfully to the scale, with mood disturbance (item 12) exerting the greatest influence on internal consistency, reflecting the importance of psychological aspects of CRS symptomatology. These findings parallel prior studies, where psychological items clustered distinctly but remained integral to overall disease burden assessment 2,11. The two-factor structure identified in our exploratory and confirmatory analyses – separating physical from psychological domains – is consistent with previous cross-cultural validations. The Portuguese 4, Hebrew 5, and Arabic 6 versions similarly supported bifactorial solutions, with psychological items clustering independently. Although the high interfactor correlation observed in our CFA (r = 0.93) suggests substantial overlap, the distinction remains clinically meaningful, aligning with the biopsychosocial model of CRS. Confirmatory factor analysis supported the proposed bifactorial structure, in line with results reported in other linguistic validations 2 and subsequent responsiveness studies 3. However, Root Mean Square Error of Approximation (RMSEA) values were inflated, likely due to the relatively small sample size and sensitivity of RMSEA to model complexity and degrees of freedom 12. Prior psychometric research has emphasised the limitations of RMSEA in small samples, recommending reliance on multiple indices for comprehensive evaluation 13. Importantly, the Italian CRS-PRO preserved discriminant validity across clinical subgroups, capturing symptom differences between CRSsNP, CRSwNP, and healthy controls. This supports its applicability in both clinical trials and routine practice, particularly in Italy, where biologic therapies for CRSwNP are being increasingly administered 14.
Despite our study supporting the strengths and cross-culturally validity of Italian CRS-PRO, we are not suggesting at present that it replaces the SNOT-22, which is in widespread use. Rather, the CRS-PRO may represent an adjunctive disease-specific measure for CRS assessment to contribute additional psychometric precision in clinical and research assessments alongside (rather than above) established instruments.
From a cross-cultural perspective, the existence of a validated Italian CRS-PRO will provide an easy-to-use instrument adapted to routine clinical practice in Italy. In the ambulatory setting, it is feasible to administer a questionnaire based on this study during the initial evaluation to quantify baseline symptom burden as well as facilitate shared decision-making for either medical or surgical therapy. The CRS-PRO may add patient-relevant information to endoscopic and radiographic findings in the preoperative clinic, but also allows for standardised tracking of symptom development and response to FESS or biologic therapy initiation during postoperative visits. Its brevity and well-disease-oriented character allow repeated use in follow-up visits to apply its longitudinal assessment, both in clinical routine and in real outcome studies. This harmonisation could contribute to standardising patient-reported outcome measurement between Italian centres and to increasing the comparability of multicentre studies.
Strengths and limitations
Strengths of this study include its prospective multicentre design, rigorous adherence to ISPOR and STROBE guidelines 9,15, and comprehensive psychometric evaluation (reliability, construct validity, factorial structure, and test–retest assessment). Limitations include the modest sample size, which may affect CFA model stability, and the lack of longitudinal responsiveness data, which could be addressed in future studies.
Conclusions
The validation of the Italian CRS-PRO provides clinicians and researchers with a concise, patient-centred, and culturally appropriate instrument. Its ability to capture both physical and psychological domains enhances its clinical utility compared with legacy tools such as the SNOT-22, which has known psychometric limitations. Future research should evaluate its responsiveness to medical and surgical interventions, ensuring its integration into routine CRS outcome assessment and international multicentre trials.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
AM: study conception and design, data collection, data analysis, manuscript drafting; LGL: data collection, manuscript revision; GF: data collection, critical revision of the manuscript; PB-R: study design, data interpretation, manuscript revision; EDC: data collection, manuscript revision; JRL: study design, data interpretation, manuscript revision; CC-H: data collection, manuscript revision; LS: data collection, manuscript revision; AMS: study conception, supervision, critical revision of the manuscript.
Ethical consideration
This study was approved by the CE A.O.U. Torino (approval number/protocol number: 00208/2024). The research was conducted ethically, with all study procedures being performed in accordance with the requirements of the World Medical Association’s Declaration of Helsinki. Written informed consent was obtained from each participant/patient for study participation and data publication
History
Received: September 14, 2025
Accepted: December 28, 2025
Figures and tables
Figure 1. Study protocol.
Figure 2. Italian version of CRS-PRO.
Figure 3. Screen plot and parallel analysis of the CRS-PRO. Eigenvalues of the CRS-PRO items are plotted against the factor number. The parallel analysis supported the retention of 2 factors, consistent with the hypothesised bifactorial structure.
Figure 4. Confirmatory factor analysis (CFA) path diagram of the two-factor model.
| Variable | Feature | Healthy | CRSsNP | CRSwNP | Total | % |
|---|---|---|---|---|---|---|
| Gender | Male | 16 | 21 | 22 | 59 | 50% |
| Female | 16 | 19 | 24 | 59 | 50% | |
| Atopy | No | 25 | 23 | 27 | 75 | 63.6% |
| Yes | 7 | 17 | 19 | 43 | 36.4% | |
| Asthma | No | 31 | 40 | 11 | 82 | 69.5% |
| Yes | 1 | 0 | 35 | 36 | 30.5% | |
| Smoking status | Never | 18 | 22 | 31 | 71 | 60.2% |
| Former | 9 | 12 | 12 | 33 | 28% | |
| Current | 5 | 6 | 3 | 14 | 11.9% | |
| Previous FESS | No | 32 | 29 | 0 | 61 | 51.7% |
| Yes | 0 | 11 | 46 | 57 | 48.3% | |
| Biologics for CRSwNP | No | 30 | 37 | 29 | 96 | 81.4% |
| Yes | 2 | 3 | 17 | 22 | 18.6% |
| Model | χ2 (df) | CFI | TLI | RMSEA (95% CI) | SRMR | Factor correlation |
|---|---|---|---|---|---|---|
| Model 1 (unidimensional) | 566(54), p < .001 | 0.977 | 0.972 | 0.285 (0.264-0.306) | 0.111 | - |
| Model 2 (two-factor: PHYS + PSY) | 555(53), p < .001 | 0.978 | 0.972 | 0.285 (0.264-0.306) | 0.109 | 0.93 |
| Reliability Analysis of the Italian CRS-PRO | ||
| Level | Cronbach’s α | McDonald’s ω |
| Total scale | 0.669 | 0.946 |
| Item-level reliability (if item deleted) | ||
| Item | Cronbach’s α if deleted | McDonald’s ω if deleted |
| CRSPRO_1_T1 | 0.646 | 0.940 |
| CRSPRO_2_T1 | 0.640 | 0.937 |
| CRSPRO_3_T1 | 0.611 | 0.942 |
| CRSPRO_4_T1 | 0.648 | 0.941 |
| CRSPRO_5_T1 | 0.634 | 0.937 |
| CRSPRO_6_T1 | 0.618 | 0.938 |
| CRSPRO_7_T1 | 0.638 | 0.940 |
| CRSPRO_8_T1 | 0.646 | 0.941 |
| CRSPRO_9_T1 | 0.635 | 0.936 |
| CRSPRO_10_T1 | 0.658 | 0.946 |
| CRSPRO_11_T1 | 0.646 | 0.944 |
| CRSPRO_12_T1 | 0.945 | 0.949 |
| Item | Factor 1 (physical) | Factor 2 (psychological) |
|---|---|---|
| CRSPRO_1_T1 | 0.71 | — |
| CRSPRO_2_T1 | 0.68 | — |
| CRSPRO_3_T1 | 0.74 | — |
| CRSPRO_4_T1 | 0.72 | — |
| CRSPRO_5_T1 | 0.69 | — |
| CRSPRO_6_T1 | 0.70 | — |
| CRSPRO_7_T1 | 0.75 | — |
| CRSPRO_8_T1 | 0.73 | — |
| CRSPRO_9_T1 | 0.71 | — |
| CRSPRO_10_T1 | — | 0.66 |
| CRSPRO_11_T1 | — | 0.69 |
| CRSPRO_12_T1 | — | 0.72 |
| Model | χ2 (df) | CFI | TLI | RMSEA (95% CI) | SRMR | Factor correlation |
|---|---|---|---|---|---|---|
| Model 1 (unidimensional) | 566(54), p < .001 | 0.977 | 0.972 | 0.285 (0.264-0.306) | 0.111 | - |
| Model 2 (two-factor: PHYS + PSY) | 555(53), p < .001 | 0.978 | 0.972 | 0.285 (0.264-0.306) | 0.109 | 0.93 |
References
- Khan A, Reaney M, Guillemin I. Development of Sinonasal Outcome Test (SNOT-22) domains in chronic rhinosinusitis with nasal polyps. Laryngoscope. 2022;132:933-941. doi:https://doi.org/10.1002/lary.29766
- Ghadersohi S, Price C, Jensen S. Development and preliminary validation of a new patient-reported outcome measure for chronic rhinosinusitis (CRS-PRO). J Allergy Clin Immunol Pract. 2020;8:2341-2350.e1. doi:https://doi.org/10.1016/j.jaip.2020.04.048
- Lin K, Price C, Huang J. Responsiveness and convergent validity of the chronic rhinosinusitis patient-reported outcome (CRS-PRO) measure in CRS patients undergoing endoscopic sinus surgery. Int Forum Allergy Rhinol. 2021;11:1308-1320. doi:https://doi.org/10.1002/alr.22782
- Sousa-Machado A, Cascão M, Sousa P. Cross-cultural validation of the Chronic Rhinosinusitis Patient-Reported Outcomes (CRS-PRO) questionnaire in Portuguese. Cureus. 2024;16. doi:https://doi.org/10.7759/cureus.74875
- Boldes T, Shehadeh R, Shavit E. Translation, cross-cultural adaptation, and validation of the Chronic Rhinosinusitis Patient-Reported Outcome (CRS-PRO) into Hebrew. J Clin Med. 2025;14. doi:https://doi.org/10.3390/jcm14072347
- Biadsee A, Abu Amsha N, Sowerby L. Validation of the Arabic Chronic Rhinosinusitis Patient-Reported Outcome (CRS-PRO): translation and cultural adaptation. Healthcare (Basel). 2025;13. doi:https://doi.org/10.3390/healthcare13030206
- Fieux M, Carsuzaa F, Charriot J. Cross-cultural adaptation of the CRS-PRO questionnaire into French. J Otolaryngol Head Neck Surg. 2023;52. doi:https://doi.org/10.1186/s40463-023-00683-0
- Maza-Solano J, García-Lliberós A, Mota-Rojas X. Cross-cultural adaptation of the CRS-PRO questionnaire into Spanish. Acta Otorrinolaringol Esp (Engl Ed). 2025;76:512-219. doi:https://doi.org/10.1016/j.otoeng.2025.512219
- von Elm E, Altman D, Egger M. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61:344-349. doi:https://doi.org/10.1016/j.jclinepi.2007.11.008
- Dunn T, Baguley T, Brunsden V. From alpha to omega: a practical solution to the pervasive problem of internal consistency estimation. Br J Psychol. 2014;105:399-412. doi:https://doi.org/10.1111/bjop.12046
- Luk L, Rotella M, Stillman L. Assessing asthma in the otolaryngologist’s office. Curr Opin Otolaryngol Head Neck Surg. 2017;25:223-230. doi:https://doi.org/10.1097/MOO.0000000000000351
- Kenny D, Kaniskan B, McCoach D. The performance of RMSEA in models with small degrees of freedom. Sociol Methods Res. 2015;44:486-507. doi:https://doi.org/10.1177/0049124114543236
- Shi D, Lee T, Maydeu-Olivares A. Understanding the model size effect on SEM Fit Indices. Educ Psychol Meas. 2019;79:310-334. doi:https://doi.org/10.1177/0013164418783530
- Bachert C, Han J, Desrosiers M. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (SINUS-24 and SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet. 2019;394:1638-1650. doi:https://doi.org/10.1016/S0140-6736(19)31881-1
- Wild D, Grove A, Martin M. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8:94-104. doi:https://doi.org/10.1111/j.1524-4733.2005.04054.x
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 308 times
- PDF downloaded - 99 times