Vestibology
Vol. 46: Issue 1 - February 2026
Italian validation of the Niigata Questionnaire to assess the severity of persistent postural-perceptual dizziness
Summary
Cover Image
Objective. The Niigata persistent postural-perceptual dizziness (PPPD) Questionnaire (NPQ), developed by Yagi et al. in 2019, assesses the severity of PPPD. Initially available in English, it was later adapted into Spanish, German, and Indian versions. This study aimed to validate the NPQ in Italian to provide a reliable tool for assessing severity of PPPD.
Materials and methods. Fifty PPPD patients (21 men, 29 women; aged 49-73) meeting diagnostic criteria were enrolled. Cross-cultural adaptation followed a standardised protocol with input from bilingual specialists and an expert committee. The questionnaire was administered during clinical evaluation and re-administered after one month, prior to treatment. Internal consistency and test–retest reliability were analysed using Cronbach’s alpha and Pearson’s correlation coefficients.
Results. Internal consistency was excellent (α = 0.95). Pearson’s correlation exceeded 0.80 for total, posture/gait, movement, and visual stimulation scores. Concordance for concentration was also high (0.999; 95% CI: 0.999-0.999).
Conclusions. The Italian NPQ is a valid and reliable instrument for quantifying PPPD severity. It can assist clinicians in diagnosis and follow-up, supporting monitoring of disease progression and effectiveness of treatment.
Introduction
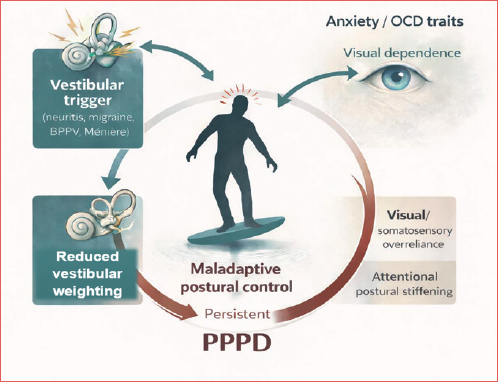
Persistent postural-perceptual dizziness (PPPD) is the most common chronic functional vestibular disorder in patients aging from 30 to 50 years, predominantly females. The estimated prevalence among patients with vestibular symptoms is 15-20%, while the incidence following acute or episodic vestibular disorders is about 25% 1. The Committee for the Classification of Vestibular Disorders of the Bárány Society defined diagnostic criteria of PPPD in 2017 establishing this condition as dizziness, instability, or non-rotational vertigo lasting 3 months or more, exacerbated by upright posture, active or passive movement, exposure to complex visual stimuli or moving3. Several triggers as peripheral or central vestibular disorders, different medical illnesses, and psychological distress can precipitate PPPD and it may be present alone or co-exist with other conditions (Cover figure). First, clinical history and then physical examination lead to diagnosis. The therapy for PPPD therapy is mainly multimodal and treatment plans include vestibular rehabilitation, pharmacological therapy, cognitive-behavioural therapy and psychotherapy. However, PPPD presents therapeutic challenges in the lack of standardised treatment options and effective tools for monitoring different therapeutic approaches.
In 2019 Yagy et al. 2 established a questionnaire to diagnose and assess the severity of PPPD: the Niigata PPPD Questionnaire (NPQ). The purpose of the NPQ is to identify the difficulties in daily life activities that patients experience due to dizziness. The PPPD is a 12-item questionnaire to assess the 3 exacerbating factors of PPPD: upright posture/walking, movement, and visual stimulation. Each factor is assessed using 4 questions. Questions 3, 6, 7 and 11 are about upright posture/walking; items 1, 5, 9 and 12 concern movement; and 2, 4, 8 and 10 concern visual stimulation. The response scores range from 0 (no discomfort) to 6 (unbearable), and thus the total score for each factor is 24 and the total final score for all three factors is 72.
In the recent years, the questionnaire has been translated and validated in various languages.
The aim of the current study is to translate and validate the NPQ in Italian in order to aid the diagnosis and assessment of PPPD severity in the Italian population.
Materials and methods
Participants
Fifty PPPD patients who met the diagnostic criteria proposed by the Bárány Society 3 were enrolled in the study. The PPPD group included 21 men and 29 women between 49 and 73 years of age. All patients were enrolled at diagnosis, before starting any treatment.
Inclusion criteria were: (a) age ranging from 30 years to 75 years; (b) diagnosis of PPPD according to the Bárány criteria; (c) attended mainstream school; (d) mastery of basic written and oral Italian. Exclusion criteria included: (a) neurological associated disease and cognitive ability impairment; (b) concomitant psychiatric conditions; (c) notable learning difficulties; (d) orthopaedic deficit affecting balance and gait; (e) illiterate.
The participant details and precipitating conditions for the PPPD patients are provided in Table I.
Prior to proceed with this study, we contacted by e-mail the authors of the NPQ to obtain the permission to translate the questionnaire who answered with an unreserved consent.
Questionnaire translation and cross-cultural adaptation
We translated in Italian and adapted the NPQ following stage by stage the guidelines of Beaton et al. 4 for the process of cross-cultural adaptation of self-report measures as performed in a previous work related to the paediatric caregiver version of the Dizziness Handicap Inventory (DHI-PC) 5.
To achieve this objective, the following methodological steps were undertaken:
- Stage I: 2 bilingual native Italian translators independently performed a forward translation of the questionnaire from English into Italian. One translator had professional expertise in translation, whereas the other possessed a medical background;
- Stage II: a consensus meeting was subsequently held between the 2 translators and the principal investigator to identify and resolve any discrepancies between the 2 translated versions, ultimately resulting in a single reconciled Italian version;
- Stage III: the reconciled version was then back-translated into English by 2 professional linguists who were blinded to the original NPQ. The purpose of this back-translation was to verify the conceptual and semantic equivalence of the translated items with the original version;
- Stage IV: an expert committee was convened, consisting of the study group, a methodologist, a language specialist, and the 2 translators. The committee conducted a comparative review of all available versions to produce a pre-final Italian version of the NPQ and prepared a written summary report;
- Stage V: the pre-final version was pilot-tested on 30 participants to evaluate item clarity and comprehensibility. These participants were excluded from the main study. Feedback indicated that all items were easily understood and that the questionnaire appropriately addressed aspects relevant to dizziness. The pilot testing also showed that administration of the adapted NPQ required approximately 10-15 minutes;
- Stage VI: finally, all preceding documentation and procedures were submitted to the original developers or coordinating committee for final review and approval of the cross-cultural adaptation process.
The 6 sequentially described steps are summarised in Figure 1.
The Italian translation of the NPQ is presented in Table II. The NPQ evaluates the degree of symptom exacerbation by the 3 characteristic factors: upright posture/walking, movement, and visual stimulation. Each factor was assessed by 4 questions; thus, there were 12 questions in the questionnaire. Q3, 6, 7, and 11 related to upright posture/walking; Q1, 5, 9, and 12 related to movement; and Q2, 4, 8, and 10 connected with the visual stimulation. Each question was scored from 0 (none) to 6 (unbearable). Finally, the total score for each factor was 24, and the total score for all 3 factors was 72.
Clinical experimentation
On the day of participation, all patients of the study underwent a comprehensive assessment that included a full medical history and neuro-otological examination, ear examination, and a basic audiological evaluation. Additionally, the adapted version of the NPQ was administered twice with an interval of one month to 50 PPPD patients who met the specified criteria for inclusion and provided written informed consent to participate in this study.
Statistical analyses
Continuous variables were expressed as means and standard deviation (numerical values and/or percentages).
Internal consistency reflects how well questionnaire items correlate with each other and measure the same construct. Internal consistency of the NPQ questionnaire was computed using Cronbach’s coefficient alpha, a numerical measure that ranges from 0 to 1. Values at least 0.7 were regarded as satisfactory.
Test-retest reliability, or reproducibility, was evaluated using Pearson’s correlation coefficient between the initial and follow-up administrations of the questionnaire. Higher correlation values indicate greater stability, suggesting that variability in scores is minimally influenced by changes in participants’ responses over time.
P values < 0.001 were considered statistically significant. Statistical analyses were performed using SPSS Version 26 (IBM Corp., Armonk, NY, USA).
Criterion validity is evaluated by the concordance correlation coefficient (Lin’s CCC), a method for measure the agreement between 2 variables. Values near +1 indicate strong concordance between the 2 measures, values near -1 indicate strong discordance, and values near 0 indicate no correlation.
Results
In our study, the majority of patients enrolled reported a history of peripheral vertigo, specifically vestibular neuritis (34%) or benign paroxysmal positional vertigo (22%). Previous head trauma was reported in 18% of cases, while 8% had a diagnosis of Menière’s disease and 8% had a history of panic disorder. Migraine was present in 6% of patients. Additionally, one patient had a prior episode of sudden deafness with acute vertigo, and another had experienced a stroke.
Internal consistency was excellent, with Cronbach’s alpha = 0.95.
Test-retest reliability for the Italian version was confirmed by Pearson’s correlation coefficient (r = 0.94, p < 0.001). A significant test-retest reliability was also found between the Italian and the English version (r = 0.95, p < 0.001).
All items showed a Pearson’s r > 0.70 in the test-retest reliability analysis. Detailed results of the reliability tests for all items are reported in Table III.
Strong concordance between repeated measures was observed across all factors. The concentration, posture/walking, movement, and visual stimulation factors showed CCC of 0.999 (95% CI: 0.999-1.000), with no ceiling or floor effects detected.
Discussion
In this study we translated into Italian the Niigata NPQ, the first instrument developed to measure the severity of PPPD. In the literature, there is a lack of other specific instruments to determine the impact of the disease in patients with PPPD.
The authors of the original article initially presented an English version of the questionnaire, which, however, had not been evaluated outside of Japan. Therefore, in 2023, Castillejos-Carrasco-Muñoz et al. 6 translated and adapted the NPQ into Spanish and studied its main psychometric properties, although they did not properly extrapolate them to other Western languages.
A revised German version was also developed in the same year7. Moreover, French 8 and Indian 9 translations have subsequently been reported in the literature.
In order to validate the questionnaire in Italian, we followed the protocol described by the authors who designed it. We also used a translation model we have previously used for vertigo in children 5.
Our results demonstrated that the NPQ was satisfactorily adapted to the Italian language, both culturally and linguistically. It demonstrated good reliability and can therefore be recommended for the management of Italian patients affected by PPPD.
Statistical analysis of our results demonstrated adequate internal consistency (alpha = 0.95). Furthermore, the good Pearson’s correlation coefficient demonstrated the test-retest reliability for the Italian version with a similar significant test-retest reliability between the Italian and English versions. This initial result confirms the validity and reliability of our translation, which carefully and rigorously followed the steps described in the literature for translation and adaptation 4.
Our data also showed a strong concordance for the posture/walking factor, the movement and the visual stimulation according to Meletaki et al.8 and Castillejos-Carrasco-Muñoz et al. 6 In Yagi’s original study 1, the Cronbach’s alpha coefficients for each NPQ factor were high except for the movement factor. This difference may be due to patient enrolment in the study by Yagi et al. 1 as not all subjects were at first diagnosis, and some had already started treatment.
In any case, we can validate the NPQ translated into Italian for both the total score and for the scores of each NPQ factor. As described by Yagi et al. 1, the questionnaire can be extremely useful for complete and efficient assessment of the different points related to the severity of PPPD. However, they believe that the NPQ is a complement to clinical diagnosis and does not replace a careful analysis of clinical history and differential diagnosis.
Diagnostic criteria for PPPD do not include specific tests, and diagnosis requires a precise assessment of symptoms and exacerbating factors. Based on our results, the NPQ is a promising questionnaire for measuring the severity of PPPD symptoms. It should be administered initially to complement clinical diagnosis and assess the severity of the condition, and used during follow-up to monitor the disease course and potential benefits of treatment.
With regard to the study’s limitations, no control group or follow-up period was included. The inclusion of a control group was avoided, as it was expected to be heterogeneous and could therefore have led to biased or misleading conclusions. Regarding follow-up, a future perspective is to determine the test-retest reliability of the NPQ after therapy.
Conclusions
A validated NPQ available in Italian can help clinicians to evaluate the severity of PPPD and the effectiveness of therapies in order to identify the best option. As well known, specific tests allowing estimation of the therapeutic effects currently do not exist, thus rendering treatment of PPPD a challenge for clinicians.
Acknowledgements
The authors wish to thank Chihiro Yagi for granting permission to perform the cross-cultural adaptation of the questionnaire. We also acknowledge the contributions of Professor Franca Cassarà and Professor Alessandra Compagnucci in the translation and methodological adaptation process.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
PMP: ideation, methodology, draft, writing, supervision and review; GR: data collection and processing, methodology, analysis, literature review, writing, editing; RR: assisted in data management; JG, ARF: critical review. All authors read and approved the last version of the manuscript.
Ethical consideration
This study was approved by Catholic University of the Sacred Heart, Rome, Italy (#0015065/23 16/05/2023) and was conducted ethically, with all study procedures being performed in accordance with the requirements of the World Medical Association’s Declaration of Helsinki. Written informed consent was obtained from each patient for study participation.
History
Received: October 27, 2025
Accepted: December 18, 2025
Figures and tables
Figure 1. Steps of the cross-cultural adaptation process according to the guidelines of Beaton et al., 2000 4.
| Characteristics | Patients (n = 50) |
|---|---|
| Age (mean) | 53.5 years |
| Gender | |
| Female, n (%) | 29 (45.2%) |
| Male, n (%) | 21 (54.8%) |
| Precipitating conditions for PPPD | |
| Vestibular neuritis | 17 (34%) |
| Benign paroxysmal positional vertigo | 11 (22%) |
| Head trauma | 9 (18%) |
| Menière’s disease | 4 (8%) |
| Panic disorder | 4 (8%) |
| Migraine | 3 (6%) |
| Sudden deafness with acute vertigo | 1 (2%) |
| Stroke | 1 (2%) |
| ISTRUZIONI: scopo del questionario è individuare le difficoltà nella vita quotidiana che possono presentarsi a causa dell’instabilità/disequilibrio. Per favore indichi la sua risposta cerchiando il numero che meglio descrive la gravità con cui ha percepito il suo problema nella scorsa settimana. Se è stato completamente impossibilitato ad eseguire qualcuna delle seguenti azioni, cerchi il numero 6. | ||
|---|---|---|
| Nessuna_______Insopportabile | ||
| Q1 | Movimenti rapidi come alzarsi o girare il capo | 0 1 2 3 4 5 6 |
| Q2 | Guardare gli scaffali in un grande negozio | 0 1 2 3 4 5 6 |
| Q3 | Camminare ad andatura regolare | 0 1 2 3 4 5 6 |
| Q4 | Guardare scene in movimento alla TV o al cinema | 0 1 2 3 4 5 6 |
| Q5 | Spostarsi in macchina, bus o treno | 0 1 2 3 4 5 6 |
| Q6 | Sedersi su una sedia senza schienale e braccioli | 0 1 2 3 4 5 6 |
| Q7 | Stare in piedi senza appoggio | 0 1 2 3 4 5 6 |
| Q8 | Guardare una schermata scorrevole sul PC o smartphone | 0 1 2 3 4 5 6 |
| Q9 | Svolgere lavori domestici o attività fisica moderata | 0 1 2 3 4 5 6 |
| Q10 | Leggere i caratteri piccoli in un libro o giornale | 0 1 2 3 4 5 6 |
| Q11 | Camminare a passo svelto | 0 1 2 3 4 5 6 |
| Q12 | Salire con l’ascensore o una scala mobile | 0 1 2 3 4 5 6 |
| r | p value | |
|---|---|---|
| Internal consistency test Cronbach’s alpha = 0.95 Test-retest correlation | ||
| Q1 | 0.87 | < 0.001 |
| Q2 | 0.87 | < 0.001 |
| Q3 | 0.80 | < 0.001 |
| Q4 | 0.90 | < 0.001 |
| Q5 | 0.76 | < 0.001 |
| Q6 | 0.88 | < 0.001 |
| Q7 | 0.82 | < 0.001 |
| Q8 | 0.78 | < 0.001 |
| Q9 | 0.95 | < 0.001 |
| Q10 | 0.84 | < 0.001 |
| Q11 | 0.86 | < 0.001 |
| Q12 | 0.82 | < 0.001 |
| Total | 0.94 | < 0.001 |
| Italian-English test-retest correlation | ||
| Q1 | 0.94 | < 0.001 |
| Q2 | 0.95 | < 0.001 |
| Q3 | 0.94 | < 0.001 |
| Q4 | 0.80 | < 0.001 |
| Q5 | 0.76 | < 0.001 |
| Q6 | 0.99 | < 0.001 |
| Q7 | 0.94 | < 0.001 |
| Q8 | 0.90 | < 0.001 |
| Q9 | 0.94 | < 0.001 |
| Q10 | 0.80 | < 0.001 |
| Q11 | 0.83 | < 0.001 |
| Q12 | 0.76 | < 0.001 |
| Total | 0.95 | < 0.001 |
References
- Madrigal J, Herrón-Arango A, Bedoya M. Persistent challenges: a comprehensive review of persistent postural-perceptual dizziness, controversies, and clinical complexities. Cureus. 2024;16. doi:https://doi.org/10.7759/cureus.60911
- Yagi C, Morita Y, Kitazawa M. A validated questionnaire to assess the severity of persistent postural-perceptual dizziness (PPPD): the Niigata PPPD Questionnaire (NPQ). Otol Neurotol. 2019;40:E747-E752. doi:https://doi.org/10.1097/MAO.0000000000002325
- Staab J, Eckhardt-Henn A, Horii A. Diagnostic criteria for persistent postural-perceptual dizziness (PPPD): Consensus document of the committee for the Classification of Vestibular Disorders of the Bárány Society. J Vestib Res. 2017;27:191-208. doi:https://doi.org/10.3233/VES-170622
- Beaton D, Bombardier C, Guillemin F. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine (Phila Pa 1976). 2000;25:3186-3191. doi:https://doi.org/10.1097/00007632-200012150-00014
- Picciotti P, Rossi G, Settimi S. Validity of Italian adaptation of the Vanderbilt Paediatric Dizziness Handicap Inventory. Acta Otorhinolaryngol Ital. 2023;43:341-347. doi:https://doi.org/10.14639/0392-100X-N2552
- Castillejos-Carrasco-Muñoz R, Peinado-Rubia A, Lérida-Ortega M. Validity and reliability of the Niigata PPPD Questionnaire in a Western population. Eur Arch Otorinolaringol. 2023;280:5267-5276. doi:https://doi.org/10.1007/s00405-023-08038-1
- Behrendt F, Stark M, Chételat S, Schädler S. The German revised version of the Niigata PPPD questionnaire (NPQ-R): development with patient interviews and an expert Delphi consensus. PLoS One. 2023;18. doi:https://doi.org/10.1371/journal.pone.0291002
- Meletaki V, Gobinet M, Léonard J. French adaptation and validation of the Niigata PPPD Questionnaire: measure of severity of persistent postural-perceptual dizziness and its association with psychiatric comorbidities and perceived handicap. Front Neurol. 2024;15. doi:https://doi.org/10.3389/fneur.2024.1388805
- Aishwarya N, Selvarajan G, Samaya K. Translation and validation of the Niigata PPPD Questionnaire into Tamil: a tool to assess persistent postural-perceptual dizziness. Indian J Otolaryngol Head Neck Surg. 2024;76:3951-3955. doi:https://doi.org/10.1007/s12070-024-04751-3
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 625 times
- PDF downloaded - 202 times