Reviews
Online First
Association between tracheo-oesophageal fistula and anti-angiogenic therapy in locally advanced/ metastatic tumours. A narrative review
Summary
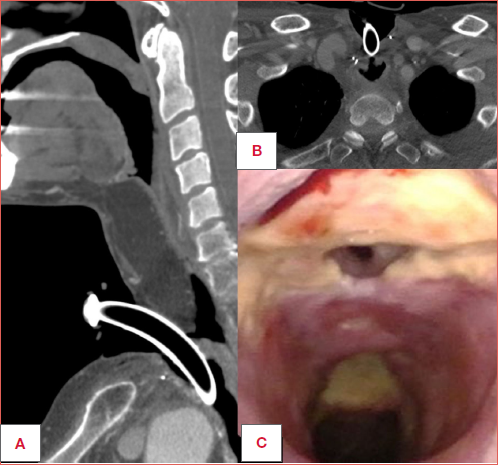
Cover Image
Anti-angiogenic therapies (AAT), including monoclonal antibodies (MAB) and tyrosine kinase inhibitors (TKI), have become a cornerstone in the management of advanced or treatment-refractory malignancies. Despite their proven efficacy, these agents can cause significant adverse effects related to impaired vascular repair and wound healing. Among the rare but serious complications, tracheoesophageal fistula (TEF) has emerged as a clinically relevant and potentially fatal event. This review analyzes the existing literature to explore the association between AAT and TEF formation, emphasizing the underlying mechanisms, risk factors, and clinical implications. Evidence suggests that inhibition of vascular endothelial growth factor signaling compromises endothelial regeneration, particularly in tissues previously exposed to radiotherapy, inflammation, or surgical manipulation. Bevacizumab-
related TEFs have been primarily reported in patients with lung cancer undergoing multimodal treatment, while TKI-associated cases, most often linked to Lenvatinib or Cabozantinib, have occurred in thyroid cancer with tracheoesophageal invasion or rapid tumor regression. No TEF has been described in treatment-naïve or neoadjuvant settings, indicating a safer profile in the absence of pre-existing local iatrogenic damage. Overall, TEF should be regarded as an extreme manifestation of wound- healing impairment rather than a random event. Careful patient selection, multidisciplinary assessment, and vigilant clinical monitoring are essential to balance therapeutic efficacy with patient safety. Further research is warranted to elucidate the biological mechanisms underlying this complication and optimize treatment strategies for high-risk patients.
Introduction
Anti-angiogenic agents represent a class of targeted therapies that act on specific molecular pathways. They work by limiting the blood supply to tumour tissue, thereby suppressing tumour growth and metastasis. The rationale is to disrupt neo-angiogenesis, a fundamental pathogenic mechanism in tumourigenesis. Although molecular and mechanistic studies have indicated that numerous regulators are engaged in tumour angiogenesis, most research on its inhibitors continues to concentrate on the vascular endothelial growth factor/receptor (VEGF/VEGFR) signalling pathway, given its central role in regulating angiogenesis. Currently, recombinant monoclonal antibodies (MAB) and small-molecule tyrosine kinase inhibitors (TKI) represent the primary classes of drugs employed in anti-angiogenic therapy (AAT) 1. MABs directed against VEGF receptors act at the upstream level of the angiogenic cascade, and TKIs block receptors phosphorylation and suppress transduction of downstream signalling pathways.
The most representative MAB is bevacizumab, which became the first FDA-approved anti-angiogenic drug in 2004 1. It significantly improved the progression-free survival of patients with renal cell carcinoma when combined with chemotherapy. In the following years, several other anti-angiogenic agents were subsequently developed and approved. In addition to MABs, TKIs were developed to inhibit VEGFRs and were initially used to improve the prognosis of patients with chronic myeloid leukaemia 2. They include a wide family of drugs that block transmembrane receptors, inhibiting angiogenesis and tumour progression. These include sorafenib and lenvatinib, orally available multi-targeted angiogenic inhibitors, approved respectively in 2005 and 2016 3-5. Although these agents act on defined molecular targets, they cannot discriminate between physiological angiogenesis, which is necessary for tissue repair, and pathological neo-angiogenesis. Hence, their mechanism of action largely accounts for the spectrum of adverse effects observed in clinical practice 6. In particular, several studies have shown that VEGF blockade damages not only neoplastic vessels but also healthy ones and results in severe problems such as haemorrhagic and thrombotic events 7,8.
It is likely that anti-VEGF drugs act in a broad and non-selective manner, affecting both tumour and healthy tissues. In contrast, studies have shown that within the category of TKIs, a further subclass exists that targets specific mutations in oncogenes or tumour suppressor genes, yielding greater selectivity and, potentially, a more favourable side-effect profile 11. Anti-angiogenic agents have shown promising outcomes in advanced or treatment-refractory malignancies, although their safety profile necessitates careful patient selection and vigilant clinical monitoring.
This review focuses on the 2 most commonly used subclasses of anti-angiogenic drugs, MABs and TKIs, with particular attention to a rare but severe complication of this therapy: the development of tracheo-oesophageal fistula (TEF). Our objective is to highlight the strength of association between TEF onset and AAT, identifying confounding or predisposing factors. We aim to provide recommendations, highlight existing knowledge gaps, and suggest strategies to better balance therapeutic efficacy with patient safety.
Side effects of anti-angiogenic agents
Multiple clinical studies have confirmed the therapeutic significance of targeting VEGF or its receptors in patients with various types of malignancies. However, anti-VEGF/VEGFR therapies are not without adverse effects and the management of these is extremely important in the optimal use of such drugs. Growing clinical experience with anti-angiogenic agents has shown that VEGF/VEGFR signalling plays critical roles in multiple organs, and that inhibiting this pathway can lead to significant adverse effects. The principal complications of anti-angiogenic agents reported in the literature include hypertension, proteinuria, hand–foot syndrome, coagulation disorder, and wound healing impairment 12-15.
Regarding arterial hypertension, the VEGF/VEGFR signaling pathway is a regulator of vasodilatation and in various trials with VEGF-A antibody and VEGFR-TKI, hypertension was the predominant, and expected, side effect 15-22. VEGF is also important in maintaining normal glomerular endothelial function. Therefore, proteinuria may be encountered in more than 30% of patients treated with bevacizumab, and is often asymptomatic 15. Additionally, hand-foot syndrome, a cutaneous rash affecting the extremities, has been commonly observed as a side effect of AAT 6. Coagulation disorders have been reported in percentages varying between 1% and 2% for thromboembolic events, and up to 6% for bleeding complications in large trials 23-26. The increased risk of bleeding and thrombosis may be explained by the physiological function of VEGF in maintaining haemostasis. VEGF supports endothelial health by promoting cell growth, protecting endothelial cells, regulating thrombotic factors, and directly affecting platelets. As a key factor in endothelial repair, VEGF is vital for maintaining vascular integrity. Its inhibition can impair cell regeneration after injury, making vessels more prone to bleeding and dysfunction. This damage exposes subendothelial collagen, activates tissue factors, and increases the risk of thrombosis. On the other hand, it is associated with treatment-induced thrombocytopenia 27-30.
Impairment of wound healing is the most important side effect of AAT for what concerns the main topic of the present review. This effect is a consequence of the mechanism explained above and represents one of the adverse effects with the greatest clinical and surgical implications. Indeed, the literature recommends discontinuation of these agents at least 5 times their terminal elimination half-life (28 hours) before elective surgery, i.e. approximately 6 days preoperatively, while resumption of therapy should be judged clinically on the basis of wound healing 31. Organ perforations and the development of TEF can be considered part of this spectrum of adverse effects. In particular, gastrointestinal perforations are widely documented in the literature 32-34, whereas TEF are encountered more sporadically and predominantly as case reports. VEGF is responsible for restoration of connective tissue and angiogenesis in injured mucosa. It is expressed mainly in the endothelial cells and connective tissue of normal intestinal mucosa. Its expression increases in both acute and chronic injury because angiogenesis, required for every repairing process, is essential for healing of gastroduodenal ulcers 15. Overexpression of VEGF is reported also after radiotherapy (RT) 35 since it exerts anti-angiogenic and anti-lymphangiogenic effects, leading to apoptosis. However, after RT there is a paradoxical increase in the expression of angiogenic growth factors, as a post-treatment defense mechanism. A study of patients with rectal cancer receiving neoadjuvant RT followed by surgery showed a significant increase in VEGF expression in post-RT specimens compared with primary tumor samples 36.
These latter 2 adverse effects are interconnected, supporting the main hypothesis that VEGF inhibition impairs the regenerative capacity of endothelial cells following any kind of tissue injury 13. These effects could be particularly evident in tissues where VEGF is overexpressed as a protective or compensatory response, and where its inhibition may therefore disrupt normal healing or defense mechanisms. Clearly, this renders tissue already subjected to any insult (inflammation, RT, surgery) less able to mount effective reparative reserves. An emblematic and extreme case is reported by Ackerman et al. 37. They reported the case of a patient receiving pharyngo-laryngectomy extended to the oesophagus and total thyroidectomy for thyroid cancer, reconstructed by a gastric pull-up with a gastro-pharyngeal anastomosis that remained stable for 23 years. After initiation of a TKI (cabozantinib) for metastatic disease, he experienced a bleeding pharyngo-cutaneous fistula at the anastomotic site, thus raising the concern that TKI initiation may have significantly contributed to wound dehiscence.
TEF in patient treated with anti-angiogenic agents
Bevacizumab
In the literature, there are limited reports 38-40 describing the development of TEF in patients receiving bevacizumab as part of treatment for lung cancer. In the report by Goodgame et al. 40, a 28-year-old patient with pulmonary adenocarcinoma was initially treated with chemo-RT. A few months after treatment, the disease progressed loco-regionally. Consequently, the therapeutic plan was switched to carboplatin, paclitaxel, and bevacizumab (15 mg/kg every 3 weeks). During treatment, at the end of the second cycle, the patient developed a peri-carinal fistula involving the right main bronchus, with a fatal outcome. The authors emphasised that the fistula appeared in a site where no evidence of disease was present.
Gore et al. 38 described a similar case: a patient with lung cancer with a recurrence after previous chemo-RT (carboplatin and paclitaxel with 66 Gy) and surgery. The patient was treated after 17 months with chemotherapy (carboplatin and gemcitabine) plus bevacizumab. At 23 days after the first cycle, the patient developed a fatal TEF.
A common feature across these cases is the use of multimodal therapy, which highlights the critical importance of careful patient selection for such regimens. Indeed, as explained before, the overexpression of VEGF after RT and the use of anti-angiogenic agents may increase the risk of side effects, in particular wound healing impairment. In 2007, Spigel et al. 39 conducted a trial enrolling patients with locally advanced non-small cell and limited-stage small cell lung cancer to assess the efficacy and safety of adding bevacizumab to chemo-RT. The trial, focusing on the occurrence of TEF, was halted early due to a relatively high incidence of this adverse event. Among the 34 patients enrolled, in fact, 4 developed TEF, one an aerodigestive haemorrhage, and another a gastrointestinal perforation. This work reinforces the role of multimodal treatment in the development of TEF, but adds another aspect: all patients who developed complications had preexisting inflammatory oesophageal disease and had undergone oesophageal dilations during treatment. It seems that 2 pathogenic factors converged: a preexisting mucosal injury with a consequent overexpression of VEGF and the impaired wound healing induced by AAT. It is possible that these events represent expected, albeit rare, complications of modern combined-modality treatment. In each instance, additional contributing factors likely played significant, if not central, roles in the development of this uncommon toxicity. Carboplatin and RT are each common in these studies.
TKIs (sorafenib, lenvatinib, and cabozantinib) in thyroid cancer
The indications for using non-selective TKIs in the management of differentiated thyroid carcinoma (DTC) are radioiodine-refractory disease without driver mutations, and neoadjuvant therapy before surgery in locally advanced disease 41. Historically, for patients not eligible for surgery, limited alternative options were available. Sorafenib and lenvatinib both showed prolonged progression-free survival in patients with radioactive iodine-refractory DTC.
The role of TKIs in thyroid cancer therapy and their association with TEF development remains an area rich in insights and controversies. First of all, in treatment of naïve patient without prior cervical or mediastinal therapy, the use of TKIs in the neoadjuvant setting has not been associated with any reported case of TEF in the literature. On the contrary, TKIs may induce significant tumour responses that facilitate less mutilating surgical approaches, potentially allowing for preservation of critical structures such as the larynx, trachea, and oesophagus 41,42. Moreover, in case of treatment of thyroid cancer, another important point is the role of tumour response to TKIs in TEF pathogenesis. It seems that significant tumour shrinkage induced by TKIs could cause TEF formation, particularly in patients whose tracheal or oesophageal walls were infiltrated by tumour at treatment initiation. Thus, it becomes challenging to discern how much of the effect is directly attributable to the drug itself, as opposed to being a consequence of the therapeutic response to tumour regression. Some reports suggest that patients with visceral infiltration at baseline should be considered at high risk for TEF when starting therapy. The average degree of tumour shrinkage leading to fistula or tumour-related bleeding was found to be 19.2% from baseline. In addition, lenvatinib-induced fistula formation and tumour-related bleeding were found to appear at 10.4 weeks with a tumour decrease of 19.2% from the start of therapy 43. Therefore, careful consideration should be applied to patients with organ invasion at baseline, as this may be a predisposing factor for TEF.
Lenvatinib
This drug is a multi-targeted TKI that inhibits the VEGFR 1-3, fibroblast growth factor receptors 1-4, and platelet-derived growth factor receptors, RET, and KIT. Despite benefit from lenvatinib, previous studies have also shown that it causes various adverse effects with a high frequency, including TEF, which indicates the need for careful management (Cover figure).
Yakota et al. 44 described a spontaneous onset of TEF in a patient treated with lenvatinib for metastatic hepatocellular carcinoma who initially received first-line therapy with atezolizumab plus bevacizumab. Upon distant progression, he underwent RT targeting the third thoracic vertebra and subsequently started lenvatinib. In this case a TEF appeared 5 months after starting the drug; it is paradigmatic for 2 reasons: the sequential use of 2 distinct anti-angiogenic agents and the development of TEF in a patient whose oesophagus and trachea were neither involved by disease nor treated by surgery. Thoracic RT remains a possible contributory factor in the development of this complication.
In the setting of laryngeal tumours, there are no reports in the literature of spontaneous TEF formation. The only case documented in the literature is reported by Salvatori et al. 45. They described a case of laryngeal adenoid cystic carcinoma who had a preexisting tracheo-oesophageal puncture (TEP) for voice rehabilitation, treated with lenvatinib and who developed increased difficulty in managing the TEP due to fistula enlargement and leakage. The authors emphasised the necessity of careful evaluation for AAT eligibility in patients with preexisting TEP. This recommendation is supported by another report 46 describing patients who underwent total laryngectomy plus TEP insertion for locally advanced thyroid tumours.
Discussion
The aim of this narrative review is to underscore the strong association between the development of TEFs and AAT, identifying potential confounding or predisposing factors. Although the literature on this subject is scarce and lacks large-scale studies, multiple case reports provide valuable experiential insights. Indeed, the evidence in the literature concerning a possible link between the use of anti-angiogenic drugs and the onset of TEF is at least suggestive. It must be emphasised that this phenomenon should be viewed as part of a broader class of complications, involving impairment of wound-healing. The mechanism, as previously described, is a non-selective inhibition of angiogenesis: this ensures suppression of neo-angiogenesis (an oncogenic mechanism), but it also causes difficulties in repairing damage, especially after (chemo-)RT, surgery or pre-existing inflammatory conditions. No cases of TEF have been reported in the literature in naïve patients or in the neoadjuvant setting, giving to neo-angiogenic agents a better safety profile. Indeed, the use of TKIs as neo-adjuvant treatment of selected cases of locally advanced DTC to reduce tumour volume and therefore morbidity of subsequent surgical resection, seems to be unrelated to TEF.
According to the available literature, gastrointestinal (GI) perforations are more frequently described than TEFs. In reports of GI perforation, patients commonly have an underlying chronic inflammatory status or previous history of abdominal RT, which predisposes them to this complication. Similarly, in all cases of TEF collected in this review, patients have a history of neck or chest RT. Probably, the higher incidence of GI perforation compared to TEF is, in our view, largely due to an epidemiological factor: it is more probable that a patient treated with anti-angiogenic drugs has a prior inflammatory GI disease than a history of cervical-mediastinal irradiation. On the other hand, the relationship between use of anti-angiogenic drugs and the development of complications such as TEF is complex and not strictly linear. This underscores the need for comprehensive, multidisciplinary assessment of the patient, beyond the oncological profile, considering anatomical, functional, surgical, and RT risk factors, as well as individual issues that may predispose to such adverse events.
Our review of the literature yields several key points to consider when selecting a patient for AAT. Although the studies in the literature did not exclude benefit in controlling disease progression despite the complications described, they emphasise the need to define eligibility criteria that ensure a favourable risk-benefit balance. According to the cases collected, particular attention should be reserved to patients with pre-existing GI or tracheo-oesophageal inflammation, previous cervico-mediastinal RT, and those with a TEP in place. In case of treatment, special attention should be taken during follow-up and pharmacovigilance. Increasing use of anti-angiogenic drugs, along with ongoing research into optimal dosing, treatment duration, and strategies to minimise and manage side effects, is expected to enhance patient tolerability and improve clinical outcomes. Nevertheless, several important questions remain unanswered and warrant further investigation. It is still unclear whether the risk of developing this complication is influenced by drug dosing, and whether a therapeutic threshold exists that allows for efficacy while minimising adverse events. The timing of onset is also a critical point: notably, these complications did not arise during the course of RT, but rather emerged in the post-treatment period, sometimes as late as 3-4 months after the end of RT.
Conclusions
AAT, particularly MABs and TKIs, have significantly expanded treatment options for patients with advanced or treatment-refractory malignancies. While their efficacy is well-documented, these agents carry a non-negligible risk of adverse effects, particularly related to impaired wound healing and tissue repair. Although rare, TEF emerges as a serious and potentially fatal complication, especially in patients with predisposing factors such as prior RT, mucosal inflammation, invasive procedures, or anatomical distortion due to tumour infiltration. Our review highlights the need for a multidisciplinary approach when considering AAT. Careful patient selection, rigorous assessment of individual risk profiles, and close clinical monitoring are essential to minimise harm while preserving therapeutic benefit. Current evidence also underscores the importance of ongoing research to clarify optimal dosing, treatment duration, and the mechanisms underlying complications like TEF.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
FEN, CM, CP: contributed to data collection, performed manuscript preparation and final edits and revisions; DM, VR, DL, CP: reviewed, contributed conceptually to the article and approved the submitted version.
Ethical consideration
No formal ethics committee approval was required for this article as it is based on already published clinical data from other studies available in the literature.
History
Received: December 8, 2025
Accepted: February 2, 2026
References
- Liu Z, Chen H, Zheng L. Angiogenic signaling pathways and anti-angiogenic therapy for cancer. Signal Transduct Target Ther. 2023;8. doi:https://doi.org/10.1038/s41392-023-01460-1
- Cohen P, Cross D, Jänne P. Kinase drug discovery 20 years after imatinib: progress and future directions. Nat Rev Drug Discov. 2021;20:551-569. doi:https://doi.org/10.1038/s41573-021-00195-4
- Escudier B, Eisen T, Stadler W. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. 2007;356:125-134. doi:https://doi.org/10.1056/NEJMoa060655
- Motzer R, Hutson T, Glen H. Lenvatinib, everolimus, and the combination in patients with metastatic renal cell carcinoma: a randomised, phase 2, open-label, multicentre trial. Lancet Oncol. 2015;16:1473-1482. doi:https://doi.org/10.1016/S1470-2045(15)00290-9
- Zirlik K, Duyster J. Anti-angiogenics: current situation and future perspectives. Oncol Res Treat. 2018;41:166-171. doi:https://doi.org/10.1159/000488087
- Cabanillas M, Takahashi S. Managing the adverse events associated with lenvatinib therapy in radioiodine-refractory differentiated thyroid cancer. Semin Oncol. 2019;46:57-64. doi:https://doi.org/10.1053/j.seminoncol.2018.11.004
- Iwasaki H, Toda S, Murayama D. Relationship between adverse events associated with lenvatinib treatment for thyroid cancer and patient prognosis. Mol Clin Oncol. 2021;14. doi:https://doi.org/10.3892/mco.2020.21908
- Verheul H, Pinedo H. Possible molecular mechanisms involved in the toxicity of angiogenesis inhibition. Nat Rev Cancer. 2007;7:475-485. doi:https://doi.org/10.1038/nrc2152
- Ratner M. Genentech discloses safety concerns over Avastin. Nat Biotechnol. 2004;22. doi:https://doi.org/10.1038/nbt1004-1198
- Kubota Y. Tumor angiogenesis and anti-angiogenic therapy. Keio J Med. 2012;61:47-56. doi:https://doi.org/10.2302/kjm.61.47
- Shyam Sunder S, Sharma U, Pokharel S. Adverse effects of tyrosine kinase inhibitors in cancer therapy: pathophysiology, mechanisms and clinical management. Signal Transduct Target Ther. 2023;8. doi:https://doi.org/10.1038/s41392-023-01469-6
- Keefe D, Bowen J, Gibson R. Noncardiac vascular toxicities of vascular endothelial growth factor inhibitors in advanced cancer: a review. Oncologist. 2011;16:432-444. doi:https://doi.org/10.1634/theoncologist.2010-0271
- Elice F, Rodeghiero F. Side effects of anti-angiogenic drugs. Thromb Res. 2012;129:S50-S53. doi:https://doi.org/10.1016/S0049-3848(12)70016-6
- Kuenen B. Analysis of prothrombotic mechanisms and endothelial perturbation during treatment with angiogenesis inhibitors. Pathophysiol Haemost Thromb. 2003;33:13-14. doi:https://doi.org/10.1159/000073281
- Roodhart J, Langenberg M, Witteveen E. The molecular basis of class side effects due to treatment with inhibitors of the VEGF/VEGFR pathway. Curr Clin Pharmacol. 2008;3:132-143. doi:https://doi.org/10.2174/157488408784293705
- Motzer R, Michaelson M, Redman B. Activity of SU11248, a multitargeted inhibitor of vascular endothelial growth factor receptor and platelet-derived growth factor receptor, in patients with metastatic renal cell carcinoma. J Clin Oncol. 2006;24:16-24. doi:https://doi.org/10.1200/JCO.2005.02.2574
- Thomas A, Morgan B, Horsfield M. Phase I study of the safety, tolerability, pharmacokinetics, and pharmacodynamics of PTK787/ZK 222584 administered twice daily in patients with advanced cancer. J Clin Oncol. 2005;23:4162-4171. doi:https://doi.org/10.1200/JCO.2005.09.034
- Wood J, Bold G, Buchdunger E. PTK787/ZK 222584, a novel and potent inhibitor of vascular endothelial growth factor receptor tyrosine kinases, impairs vascular endothelial growth factor-induced responses and tumor growth after oral administration. Cancer Res. 2000;60:2178-2189.
- Rugo H, Herbst R, Liu G. Phase I trial of the oral antiangiogenesis agent AG-013736 in patients with advanced solid tumors: pharmacokinetic and clinical results. J Clin Oncol. 2005;23:5474-5483. doi:https://doi.org/10.1200/JCO.2005.04.19220
- Heymach J, Desai J, Manola J. Phase II study of the antiangiogenic agent SU5416 in patients with advanced soft tissue sarcomas. Clin Cancer Res. 2004;10:5732-5740. doi:https://doi.org/10.1158/1078-0432.CCR-04-015721
- Fiedler W, Serve H, Döhner H. A phase 1 study of SU11248 in the treatment of patients with refractory or resistant acute myeloid leukemia (AML) or not amenable to conventional therapy for the disease. Blood. 2005;105:986-993. doi:https://doi.org/10.1182/blood-2004-05-184622
- Veronese M, Mosenkis A, Flaherty K. Mechanisms of hypertension associated with BAY 43-9006. J Clin Oncol. 2006;24:1363-1369. doi:https://doi.org/10.1200/JCO.2005.02.0503
- Kabbinavar F, Hambleton J, Mass R. Combined analysis of efficacy: the addition of bevacizumab to fluorouracil/leucovorin improves survival for patients with metastatic colorectal cancer. J Clin Oncol. 2005;23:3706-3712. doi:https://doi.org/10.1200/JCO.2005.00.232
- Hedrick E, Kozloff M, Hainsworth J. Safety of bevacizumab plus chemotherapy as first-line treatment of patients with metastatic colorectal cancer: updated results from a large observational registry in the US (BRiTE). J Clin Oncol. 2006;11.
- Berry S, Cunningham D, Michael M. Preliminary safety of bevacizumab with first-line Folfox, Capox, Folfiri and capecitabine for mCRC – First B.E.A.Trial. J Clin Oncol. 2006;11.
- Hurwitz H, Fehrenbacher L, Hainsworth J. Bevacizumab in combination with fluorouracil and leucovorin: an active regimen for first-line metastatic colorectal cancer. J Clin Oncol. 2005;23:3502-3508. doi:https://doi.org/10.1200/JCO.2005.10.017
- Kuenen B, Levi M, Meijers J. Potential role of platelets in endothelial damage observed during treatment with cisplatin, gemcitabine, and the angiogenesis inhibitor SU5416. J Clin Oncol. 2003;21:2192-2198. doi:https://doi.org/10.1200/JCO.2003.08.04628
- Zachary I. VEGF signalling: integration and multi-tasking in endothelial cell biology. Biochem Soc Trans. 2003;31:1171-1177. doi:https://doi.org/10.1042/bst031117129
- Zachary I. Signaling mechanisms mediating vascular protective actions of vascular endothelial growth factor. Am J Physiol Cell Physiol. 2001;280:C1375-C1386. doi:https://doi.org/10.1152/ajpcell.2001.280.6.C137530
- Kilickap S, Abali H, Celik I. Bevacizumab, bleeding, thrombosis, and warfarin. J Clin Oncol. 2003;21:3542-3543. doi:https://doi.org/10.1200/JCO.2003.99.04631
- Cheng C, Nayernama A, Christopher Jones S. Wound healing complications with lenvatinib identified in a pharmacovigilance database. J Oncol Pharm Pract. 2019;25:1817-1822. doi:https://doi.org/10.1177/107815521881710932
- Hartl D, Guerlain J, Bresuskin I. Surgery in the context of kinase inhibitor therapy for locally invasive thyroid cancer. Eur J Surg Oncol. 2020;46:650-655. doi:https://doi.org/10.1016/j.ejso.2019.09.18433
- Zhou J, Wei Z, Zheng Y. Disproportionality analysis of lenvatinib-caused gastrointestinal perforation in cancer patients: a pharmacovigilance analysis based on the US food and drug administration adverse event reporting system. J Clin Pharmacol. 2023;63:1133-1140. doi:https://doi.org/10.1002/jcph.231234
- Wichelmann T, Abdulmujeeb S, Ehrenpreis E. Bevacizumab and gastrointestinal perforations: a review from the FDA adverse event reporting system (FAERS) database. Aliment Pharmacol Ther. 2021;54:1290-1297. doi:https://doi.org/10.1111/apt.1660135
- Chen Y, Pan S, Wang J. Radiation-induced VEGF-C expression and endothelial cell proliferation in lung cancer. Strahlenther Onkol. 2014;190:1154-1162. doi:https://doi.org/10.1007/s00066-014-0708-z36
- Nozue M, Isaka N, Fukao K. Over-expression of vascular endothelial growth factor after preoperative radiation therapy for rectal cancer. Oncol Rep. 2001;8:1247-1249. doi:https://doi.org/10.3892/or.8.6.124737
- Ackerman J, Kent S, Walker P. Gastropharyngeal anastomotic leak in medullary thyroid carcinoma following initiation of a tyrosine kinase inhibitor: a case report of an unusual side effect of cabozantinib. Ann Otol Rhinol Laryngol. 2020;129:657-661. doi:https://doi.org/10.1177/0003489420902161
- Gore E, Currey A, Choong N. Tracheoesophageal fistula associated with bevacizumab 21 months after completion of radiation therapy. J Thorac Oncol. 2009;4:1590-1591. doi:https://doi.org/10.1097/JTO.0b013e3181c06a6f39
- Spigel D, Hainsworth J, Yardley D. Tracheoesophageal fistula formation in patients with lung cancer treated with chemoradiation and bevacizumab. J Clin Oncol. 2010;28:43-48. doi:https://doi.org/10.1200/JCO.2009.24.735340
- Goodgame B, Veeramachaneni N, Patterson A. Tracheo-esophageal fistula with bevacizumab after mediastinal radiation. J Thorac Oncol. 2008;3:1080-1081. doi:https://doi.org/10.1097/JTO.0b013e3181858eba41
- Stewart K, Strachan M, Srinivasan D. Tyrosine kinase inhibitor therapy in locally advanced differentiated thyroid cancer: a case report. Eur Thyroid J. 2019;8:102-107. doi:https://doi.org/10.1159/000494880
- Alshehri K, Alqurashi Y, Merdad M. Neoadjuvant lenvatinib for inoperable thyroid cancer: a case report and literature review. Cancer Rep (Hoboken). 2022;5. doi:https://doi.org/10.1002/cnr2.146643
- Staub Y, Nishiyama A, Suga Y. Clinical characteristics associated with lenvatinib-induced fistula and tumor-related bleeding in patients with thyroid cancer. Anticancer Res. 2019;39:3871-3878. doi:https://doi.org/10.21873/anticanres.1353744
- Yokota K, Kitagawa H, Okamoto K. A case of tracheoesophageal fistula in a non-metastatic site during lenvatinib treatment for hepatocellular carcinoma. Cancer Diagn Progn. 2023;3:475-478. doi:https://doi.org/10.21873/cdp.1024245
- Salvatori S, Tanvetyanon T. Fatal tracheoesophageal puncture leakage associated with lenvatinib. Cureus. 2023;15. doi:https://doi.org/10.7759/cureus.4349046
- Britt C, Russell J. Tyrosine kinase inhibitor use and wound healing in tracheoesophageal punctures. Ear Nose Throat J. 2019;98:510-512. doi:https://doi.org/10.1177/014556131983980547
- Blevins D, Dadu R, Hu M. Aerodigestive fistula formation as a rare side effect of antiangiogenic tyrosine kinase inhibitor therapy for thyroid cancer. Thyroid. 2014;24:918-922. doi:https://doi.org/10.1089/thy.2012.059848
- Valerio L, Giani C, Agate L. Prevalence and risk factors of developing fistula or organ perforation in patients treated with lenvatinib for radioiodine-refractory thyroid cancer. Eur Thyroid J. 2021;10:399-407. doi:https://doi.org/10.1159/00051418249
- Temperley T, Temperley H, O’Sullivan N. Tracheoesophageal fistula development following radiotherapy and tyrosine kinase inhibitors in a patient with advanced follicular thyroid carcinoma: a case-based review. Ir J Med Sci. 2024;193:1143-1147. doi:https://doi.org/10.1007/s11845-023-03559-450
- Soria J, Deutsch E. Hemorrhage caused by antiangiogenic therapy within previously irradiated areas: expected consequence of tumor shrinkage or a warning for antiangiogenic agents combined to radiotherapy?. Ann Oncol. 2011;22:1247-1249. doi:https://doi.org/10.1093/annonc/mdq775
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2024 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 383 times
- PDF downloaded - 134 times