Annual congress report
Vol. 46: 112 TH CONGRESS SIOECHCF - OFFICIAL REPORT 2026
Margin burden and postoperative management after transoral laser microsurgery for laryngeal glottic squamous cell carcinoma: a multicentre retrospective study on 1216 patients
Summary
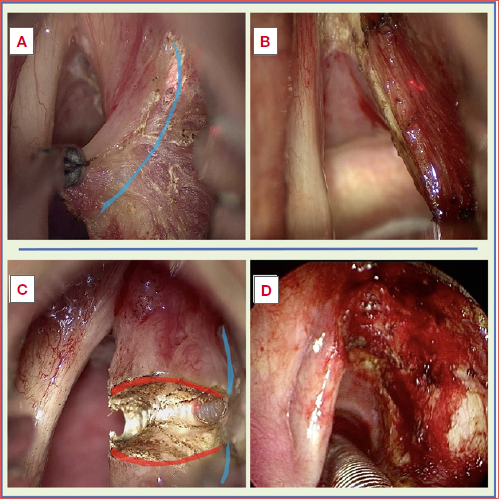
Cover Image
Objective. To evaluate the prognostic impact of surgical margin burden and postoperative management after transoral laser microsurgery (TOLMS) for glottic laryngeal squamous cell carcinoma (LSCC) in a large multicentre cohort.
Methods. A retrospective multicentre study included 1216 patients with pT1-pT3 LSCC treated with TOLMS. Surgical margins were classified as free, single superficial positive, multiple superficial positive, or deep positive. Disease-free survival (DFS), disease-specific survival (DSS), and overall survival (OS) were analysed using Kaplan-Meier estimates and multivariable Cox models, accounting for pathological stage and postoperative management.
Results. Pathological T category was independently associated with DFS and DSS. A single superficial positive margin showed DFS comparable to free margins. Multiple superficial positive margins were associated with increased recurrence risk, while deep margin involvement was strongly associated with both recurrence (hazard ratio [HR] 3.96) and disease-specific mortality (HR 6.82). Among patients with positive margins, second-look surgery achieved better DFS than postoperative radiotherapy or surveillance. Residual carcinoma at revision surgery was a major predictor of poor DFS and DSS.
Conclusions. After TOLMS, oncologic risk is driven by margin type and burden rather than margin positivity alone. Deep margin involvement and residual disease identify patients requiring intensified management, supporting a risk-adapted postoperative strategy.
Introduction
Laryngeal squamous cell carcinoma (LSCC) represents a distinctive malignancy within head and neck oncology, owing to its anatomical complexity and the critical role of the larynx in phonation, respiration, and swallowing. Although LSCC is relatively uncommon, with an incidence that increases steadily with age and peaks in older adults, global survival outcomes have improved over recent decades. This progress has been attributed to earlier diagnosis and the increasing adoption of surgical organ-preserving treatment strategies aimed at maintaining oncologic control while minimizing functional morbidity 1-3.
Among surgical larynx-preservation approaches, transoral laser microsurgery (TOLMS) has become a cornerstone in the management of early and selected intermediate-stage LSCC. When performed in experienced centres and in appropriately selected patients, TOLMS provides excellent local control and disease-specific survival (DSS), with favorable functional outcomes compared with open surgery or total laryngectomy, even in intermediate-stage LSCC 4. Consequently, TOLMS is now widely incorporated into contemporary treatment algorithms for glottic and selected supraglottic cancers 5.
Within this context, surgical margin status remains a pivotal prognostic factor following TOLMS. However, margin assessment in TOLMS is intrinsically challenging because of specimen fragmentation, tissue shrinkage, thermal artifacts, and subsite-specific anatomical constraints 6. A recent systematic review and meta-analysis confirmed that positive margins are associated with inferior oncologic outcomes, including higher risks of local recurrence, worse disease-free survival (DFS), and disease-specific mortality 7. Nevertheless, substantial heterogeneity persists across studies with respect to margin definitions, pathological reporting, and postoperative management strategies.
Importantly, accumulating evidence suggests that not all margin involvements carry the same prognostic weight. Several retrospective series have demonstrated that a single superficial positive margin, particularly in early-stage disease, does not uniformly translate into worse oncologic outcomes and may be safely managed with close endoscopic surveillance in selected cases 8-10. In contrast, deep margin involvement and/or multiple positive margins are consistently associated with a higher risk of local failure and often prompt additional treatment, such as redo surgery or adjuvant radiotherapy (RT) 8-10. Moreover, the action taken in case of close/uncertain margins is arbitrary, with some treating them as positive and others as negative margins. The literature describes close margins as being associated with a higher risk of local recurrence, which does not always translate into lower specific survival 11,12. This risk-stratified interpretation of margins has been further reinforced by recent international consensus statements, which emphasize individualised postoperative decision-making based on margin type, margin burden, tumour characteristics, and patient-related factors rather than a purely binary margin classification 13.
Despite an expanding body of literature, evidence on margin status after TOLMS still largely derives from single-institution retrospective series, characterised by heterogeneous definitions and inconsistent postoperative strategies. As a result, the prognostic meaning of different positive-margin patterns and their optimal management remain highly variable and poorly standardised across centres, generating persistent uncertainty in daily clinical practice.
In this multicentric study, we aim to evaluate the prognostic significance of surgical margin status after TOLMS for glottic LSCC using a standardised, risk-oriented margin classification, also accounting for real-world postoperative management strategies. By leveraging a large, multi-institutional cohort, this work seeks to clarify the differential impact of superficial vs deep and single vs multiple margin involvement, thereby providing clinically actionable evidence to refine postoperative decision-making beyond the existing single-centre literature.
Materials and methods
Study design and population
This retrospective study included patients with LSCC treated with TOLMS between January 2000 and October 2025 at 3 tertiary referral centres for otolaryngology and head and neck cancer: the European Institute of Oncology (IEO), IRCCS, Milan; IRCCS Ospedale Policlinico San Martino, Genoa; and Hospital Clínic, University of Barcelona.
Adult patients (≥ 18 years) with histologically confirmed SCC staged pT1-pT3 according to the 8th edition of the TNM Classification of Malignant Tumors 14, without clinical evidence of cervical lymph node or distant metastases (cN0, M0), and treated with curative intent were eligible. Written informed consent for the scientific use of clinical data was required.
Patients were excluded if they had undergone prior laryngeal surgery or RT, had an excisional biopsy performed at another institution resulting in pT0 status, had laryngeal dysplasia or carcinoma in situ, showed evidence of persistent disease within 3 months after treatment, were younger than 18 years, or declined consent.
Demographic, clinical, radiological, treatment-related, and outcome data were retrospectively collected, including age, gender, smoking and alcohol history, preoperative imaging, surgical procedure classified according to the European Laryngological Society (ELS) classification, administration of adjuvant therapies or need for second-look surgery (SLS), oncologic outcomes (recurrence and survival), salvage treatments, and status at last follow-up 15,16. Histopathological reports were reviewed to assess tumour infiltration patterns, namely involvement of the subepithelial connective tissue, vocalis muscle, anterior or posterior paraglottic space, anterior commissure, and supra- or subglottic extension, as well as final margin status.
Surgical margins were systematically classified as free, close, or positive based on histopathological assessment. Margins were defined as free when the distance between the tumour and the resection edge was ≥ 1 mm, close when the distance was < 1 mm, and positive in the presence of SCC at the resection margin. In cases of margin involvement, the number of positive margins and their anatomical location were recorded, distinguishing between superficial and deep margins.
In cases of deep or multiple superficial positive margins, or when suspicious findings emerged after completion of the healing phase, SLS was performed within 4-6 weeks of the initial procedure. Indications for adjuvant treatment were discussed by a multidisciplinary tumour board. Deviations from the planned therapeutic strategy were primarily related to patient refusal or medical contraindications precluding additional treatment; in such cases, patients were managed with a strict surveillance protocol. Otherwise, follow-up was scheduled in accordance with the ELS guidelines 17.
Statistical analysis
Continuous variables were summarised as median and interquartile range (IQR) or mean and standard deviation (SD), as appropriate, while categorical variables were reported as counts and percentages. Comparisons between groups were performed using the χ2 test or Fisher’s exact test for categorical variables, and the Student’s t test or Mann-Whitney U test for continuous variables, according to data distribution.
Oncologic endpoints included overall survival (OS), DFS, and DSS. OS was defined as the time from surgery to death (any cause), DFS as the time from surgery to disease recurrence (any type of recurrence), and DSS as the time from surgery to death from disease. Survival curves were estimated using the Kaplan-Meier method and compared using the log-rank test. Although laryngectomy-free survival (LFS) was initially considered as an outcome of interest, the low number of events resulted in limited statistical power. A post hoc power analysis showed an estimated power of approximately 18%; therefore, formal time-to-event analyses for LFS were not pursued, and laryngeal preservation was reported descriptively as the final laryngeal preservation rate.
Univariable and multivariable Cox proportional hazards regression models were used to assess the association between clinicopathological variables and survival outcomes. For margin-related analyses, close and free margins were grouped into a single category and compared against positive margins, after preliminary Kaplan-Meier analyses indicated that this categorisation provided the best balance between model stability and clinical relevance. In all analyses, patients with free margins who underwent radical TOLMS and postoperative surveillance were used as the reference category.
To further evaluate the oncologic risk associated with surgical margin status, dedicated analyses focused on patients with positive margins who deviated from the planned postoperative protocol and were managed with surveillance alone. Within this subgroup, margin status was further characterised according to the number of involved margins and their anatomical type (superficial vs deep), allowing assessment of survival outcomes in patients whose oncologic course was driven by residual disease without additional surgical or adjuvant treatment.
Variables included in multivariable models were selected a priori based on clinical relevance. The proportional hazards assumption was evaluated using Schoenfeld residuals and further assessed by fitting time-dependent effects through polynomial regression of scaled Schoenfeld residuals. Model diagnostics were performed to verify the adequacy of the fitted models.
All statistical tests were two-sided, and a p value < 0.05 was considered statistically significant. Statistical analyses were conducted using dedicated statistical software (R Foundation for Statistical Computing, Vienna, Austria; and Jamovi, The Jamovi Project).
Results
A total of 1216 patients treated with TOLMS for glottic LSCC were included (IEO, n = 674; San Martino, n = 447; Hospital Clínic, n = 95). The cohort was predominantly males (90%) and smokers (78%), with a median age of 66 years (IQR 59-74) (Tab. I). Pathological stage was pT1 in 57%, pT2 in 28%, and pT3 in 15%. Final margins were free in 63% and positive in 37%. Postoperative management included follow-up alone (63%), SLS (17%), adjuvant therapy (5.9%), combined SLS and adjuvant therapy (1.2%), and surveillance despite positive margins (12%). Residual carcinoma was identified in 61 patients (27% of revision surgeries). At last follow-up, 80% were alive with no evidence of disease, 14% had died from other causes, and 5% had died of disease; total laryngectomy was required in 5.3%.
Survival analysis
At initial Kaplan-Meier analyses stratified by pT category, surgical margin status, and postoperative management, survival curves showed progressive separation across increasing categories for OS, DFS, and DSS (log-rank p < 0.001). Patients with pT1 disease had the most favourable survival, followed by pT2 and pT3 tumors. Across endpoints, patients with free margins consistently showed higher survival probabilities than those with positive margins (Fig. 1A-F).
Given the known technical challenges associated with tumors involving the anterior commissure, we further explored the relationship between pathologic tumour extent, anterior commissure involvement, and the risk of positive margins. In univariate logistic regression, anterior commissure involvement was associated with an increased likelihood of positive margins (OR 1.47, 95% CI 1.05-2.06; p = 0.03). However, in multivariable analysis, this association was no longer significant after adjustment for pT category, with pathologic T category emerging as the dominant predictor of margin positivity (OR 4.56, 95% CI 3.13-6.65; p < 0.001), suggesting that the increased risk attributed to anterior commissure involvement is largely mediated by greater tumour extent rather than by anatomical site alone.
Stratification by postoperative management revealed distinct survival patterns. Patients managed with follow-up alone after radical TOLMS in first instance, showed higher survival probabilities, whereas those undergoing combined SLS with adjuvant treatment displayed progressively lower survival estimates, with this latter subgroup showing the lowest DFS and DSS over time (Fig. 2A-B).
In multivariable analyses, pathological T category was independently associated with recurrence risk and DSS. For DFS, compared with pT1 tumours, pT2 had a HR of 2.49 (95% CI 1.69-3.66; p < 0.001) and pT3 a HR of 4.33 (95% CI 2.83-6.62; p < 0.001). For DSS, pT2 tumours showed a HR of 2.18 (95% CI 1.08-4.88; p = 0.003), and pT3 a HR of 4.68 (95% CI 2.02-10.82; p < 0.001)
When surgical margins were examined in the multivariable analysis, patients with one superficial positive margin showed DFS comparable to free margins (HR 1.39, 95% CI 0.74-2.62; p = 0.302). In contrast, patients with > 1 superficial positive margin exhibited an increased recurrence risk (HR 2.31, 95% CI 0.99-5.48), reaching borderline statistical significance (p = 0.055). Deep margin involvement was associated with a markedly higher recurrence risk (HR 3.96, 95% CI 2.22-7.03; p < 0.001).
For DSS, deep margin involvement emerged as the only margin-related factor significantly associated with disease-specific mortality (HR 6.82, 95% CI 2.71-17.14; p < 0.001), whereas superficial margin involvement, both as single or multiple, was not (HR 1.72, 95% CI 0.49-5.98; p = 0.394). Age was not associated with DFS or DSS (p > 0.05) but was significantly associated with OS (p < 0.05).
Overall, these findings delineated a progressive gradient of recurrence risk from free margins and one superficial involved, to > 1 superficial margins, and ultimately to deep margin involvement, corroborated by adjusted DFS curves. Adjusted DSS curves confirmed the distinct prognostic role of deep margin involvement (Fig. 3A-B).
To evaluate postoperative management in patients with positive margins, multivariable Cox models were fitted accounting for collinearity between margin status and treatment by stratifying the baseline hazard according to margin type (free, superficial, deep). In these models, pT categories remained independently associated with DFS and DSS (p < 0.05).
Using radical surgery (free/close margins) as the reference category, postoperative management strategies delineated distinct oncologic trajectories in multivariable Cox models. Patients undergoing SLS with negative final histopathology – reflecting successful re-radicalisation – showed no significant differences in DFS or DSS compared with the reference group.
Among patients with residual carcinoma at SLS, divergent patterns emerged according to subsequent management. Patients managed with surveillance exhibited the highest risks of both recurrence (DFS: HR 3.96, 95% CI 2.46-6.29; p < 0.001) and disease-specific death (DSS: HR 5.04, 95% CI 2.18-11.68; p < 0.001). In contrast, patients receiving adjuvant therapy after SLS did not show a statistically significant increase in recurrence risk, suggesting a partial mitigation of disease progression; however, their risk of disease-specific mortality remained markedly elevated (DSS: HR 4.37, 95% CI 1.24-15.45; p = 0.022) (Fig. 4A-B).
Discussion
In this large cohort of 1216 patients treated with TOLMS for pT1-pT3 glottic LSCC, we provide robust multicentre evidence supporting a granular, risk-oriented evaluation of surgical margins and postoperative management.
In all analyses, pT category showed a strong, independent association with both DFS and DSS, with a clear stepwise gradient from pT1 to pT3 tumours. This finding is fully consistent with the existing literature and reinforces the concept that local tumour extension remains the cornerstone of oncologic risk stratification in LSCC. Large single-centre and multicentre series have consistently demonstrated inferior outcomes for pT2 and pT3 tumour compared with pT1 lesions after TOLMS. Marchi et al. in a multicentric study of 637 pT2-pT3 glottic cancers, reported significantly worse local control and DSS in tumours involving the paraglottic space, particularly posterior paraglottic space involvement, despite uniform surgical strategies 4. Furthermore, other authors have repeatedly shown that tumour location, depth of infiltration and three-dimensional tumour spread, rather than TNM category alone, drive recurrence risk after TOLMS 4,18.
Our findings not only confirm these observations in a broader, real-world multicentre cohort, but also strengthen them by demonstrating, within a single analytical framework, that margin-related effects remain independent from pT category.
The central contribution of the present study lies in its nuanced analysis of different margin burden.
While margin positivity has traditionally been considered an adverse prognostic factor, our data clearly quantify the different hazards associated with the number and type of positive margins.
Patients with a single superficial positive margin exhibited DFS fully comparable to those with free margins, with no signal of clinically meaningful increase in recurrence risk (p > 0.05). This aligns closely with prior evidence suggesting that superficial margin involvement, particularly when isolated, often reflects technical and pathological artifacts rather than true residual disease. Fiz et al. reported that up to 80% of close/superficial margins after TOLMS may be false positives, largely due to laser-induced thermal damage, specimen shrinkage, and orientation difficulties 19 (Cover figure).
Our data reveal a clear biological gradient of recurrence risk with increasing superficial margin burden (> 1 superficial positive margin). This gradient supports a quantitative interpretation of margin involvement, in line with the concept of “margin burden” proposed in several contemporary reviews and consensus statements, while providing, for the first time, a data-driven quantification of the associated oncologic risk. These findings indeed extend previous observations suggesting a limited prognostic impact of isolated superficial margin involvement 8,10,19,20 into a robust multicentre framework.
Deep margin involvement emerged as the most clinically relevant and statistically robust variable in our analysis. Patients with deep positive margins showed a nearly 4-fold increased risk of recurrence and a more than 6-fold increased risk of disease-specific death, independent of pT category. These findings are in strong agreement with previous literature. Fiz et al. and Vander Poorten et al. both emphasised that deep margin positivity, particularly when associated with multiple involved margins, represents a true oncologic risk and generally warrants additional treatment, preferring SLS when feasible over RT 10,21.
Notably, recent meta-analyses addressing margin status after TOLMS have yielded heterogeneous results. De Virgilio et al. reported an association between positive margins and worse local control and survival, but also highlighted substantial variability in margin definitions and postoperative management7. Iandelli et al. found that positive margins were associated with an aHR for OS of 1.30, with wide CI crossing unity, underscoring the difficulty of interpreting margins without stratification by type and burden 22.
Our data help reconcile these discrepancies by providing strong multicentre evidence that deep margin involvement is the true driver of disease-specific mortality after TOLMS.
Another key finding of this study concerns the role of postoperative management strategies in patients with positive margins. Patients managed with SLS generally experienced better DFS than those treated with adjuvant RT or surveillance alone, although DSS remained inferior to that of patients achieving primary surgical radicality. Importantly, patients managed with adjuvant therapy or surveillance despite positive margins likely represent intrinsically higher-risk categories, reflecting greater tumour burden or technical constraints limiting further endoscopic resection.
These findings are closely aligned with earlier single-institution evidence, who had already questioned the true protective role of postoperative RT following TOLMS for early-intermediate glottic cancer 10. In that experience, adjuvant RT failed to demonstrate a clear advantage over SLS in terms of local control, suggesting that RT alone may be insufficient to compensate for incomplete surgical radicality. Importantly, it was also emphasised that the risk of positive margins is not driven by anatomical subsite per se, but rather by the combined effect of tumour burden and technical factors, including laryngeal exposure, with the apparent impact of anterior commissure involvement largely mediated by pathologic T category.
When stratified by margin type, our data identify SLS as the key survival discriminator, being associated with favourable outcomes when there is no evidence of residual disease after radicalisation, whereas its prognostic value collapses in the presence of residual carcinoma.
Indeed, patients with histologically confirmed residual disease at SLS showed DFS and DSS comparable to those treated with SLS plus adjuvant therapy, and markedly worse than patients with negative re-resection, supporting a clear prognostic distinction between false-positive margins and true residual tumour.
This risk-based framework closely mirrors the pragmatic algorithm proposed by Vander Poorten et al. 21, in which isolated superficial margin involvement may be managed with intensified follow-up, whereas multiple superficial or deep positive margins warrant additional action, preferentially SLS, reserving postoperative RT for cases in which negative re-resection is unlikely or residual/multifocal disease persists 21,23. In more advanced disease, these findings intersect with the evidence summarised by Pinacoli et al. in pT3 glottic cancers treated by TOLMS, where postoperative (chemo)RT was associated with improved local control and DFS 24. Importantly, however, that analysis focused on the impact of adjuvant treatment after primary TOLMS and did not specifically address the prognostic role of SLS or the biological implications of residual disease. As such, the management of failed endoscopic radicality remained beyond the scope of that study.
Our data expand this framework by introducing a dynamic, pathway-based interpretation of postoperative management. In patients undergoing SLS, negative histopathological findings (no residual disease) effectively show similar prognosis to that of patients with free margins.
Residual carcinoma at SLS identified a subgroup with an unfavourable oncologic profile, mostly represented by patients with initially pT2-3 disease and profound deep margin involvement.
Adjuvant therapy was associated with improved DFS, although this did not translate into directly improved DSS. In this context, residual carcinoma after SLS may indicate limited endoscopic oncologic control in selected high-risk patients rather than inadequate postoperative treatment intensity. In such cases, early multidisciplinary evaluation, including consideration of alternative surgical strategies, may be appropriate within a risk-adapted, patient-centred framework.
The retrospective design and the inherent heterogeneity of postoperative management across centres represent unavoidable limitations. Although multivariable and stratified analyses were used to mitigate confounding, residual selection bias cannot be excluded. Additionally, margin assessment remains dependent on pathological interpretation, which may vary across institutions despite shared definitions.
Conclusions
This multicentre study demonstrates that the prognostic impact of surgical margins after TOLMS for glottic LSCC is driven primarily by margin type and burden rather than by margin positivity alone. Deep margin involvement and residual carcinoma at SLS are the key determinants of recurrence and disease-specific mortality. These findings strongly support a risk-adapted, individualised more aggressive postoperative strategy, consistent with contemporary international consensus, and provide solid basis for refining clinical decision-making after TOLMS in high-risk patients (Tab. II).
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This work was partially supported by the Ministry of Health, Italy with Ricerca Corrente and 5 × 1000 funds.
Author contributions
FC, EB, CS, MT, MF, CM, GA, RDR, FXAJ, VDP: data collection; FM, FC, IV, GT, GP, MA study design; FC, EB, SFZ, JMC, FM, JLP: drafting the manuscript; FC, FM, IV, GP, MA: revision of the manuscript.
Ethical consideration
This study was approved by the Institutional Ethics Committee (IEO_UID 3563; ID LAR_MULTI).
The research was conducted ethically, with all study procedures being performed in accordance with the requirements of the World Medical Association’s Declaration of Helsinki.
Written informed consent was obtained from each participant/patient for study participation and data publication.
History
Received: January 29, 2026
Accepted: March 16, 2026
Figures and tables
Figure 1. A-F) Kaplan-Meier survival curves stratified by pathological T category and margin status. Panels A and D show disease-free survival (DFS); panels B and E show disease-specific survival (DSS); panels C and F show overall survival (OS). Panels A-C are stratified by pathological T category (pT1, pT2, pT3), demonstrating a stepwise worsening of DFS, DSS, and OS with increasing tumour category. Panels D-F are stratified by margin status after surgery, also showing worse survival outcomes in patients with positive margins compared to radical surgery.
Figure 2. A-B) Cumulative hazard curves from Cox proportional hazards models according to postoperative management after TOLMS. Panel A shows cancer-related mortality and panel B tumour recurrence. Follow-up after free margins was associated with the lowest cumulative hazards, whereas combined second-look plus adjuvant treatment had worse outcomes.
Figure 3. A-B) Adjusted survival curves derived from Cox proportional hazards models according to surgical margin type. Panel A shows disease-free survival, and panel B disease-specific survival. Margins are classified as free, single superficial positive, multiple superficial positive, and deep positive. Survival estimates are adjusted using average covariate values. Deep margin involvement is associated with markedly worse outcomes, whereas single superficial involvement shows survival comparable to free margins.
Figure 4. A-B) Multivariable Cox proportional hazards models for oncologic outcomes. Panel A shows hazard ratios for disease-free survival, and Panel B for disease-specific survival. Models were stratified by margin status (superficial, deep) and adjusted for pathologic tumour category, postoperative management, and presence of residual carcinoma at second-look surgery. Squares indicate point estimates and horizontal bars represent 95% confidence intervals; the vertical dashed line denotes the null effect (HR = 1). CI: confidence interval; DFS: disease-free survival; DSS: disease-specific survival; HR: hazard ratio; pT: pathologic tumour category; SLS: second-look surgery.
| Characteristic | N = 1216 |
|---|---|
| Gender | |
| Female | 126 (10%) |
| Male | 1090 (90%) |
| Age | 66 (59, 74) |
| Smoke | 922 (78%) |
| Unknown | 32 |
| Alcohol | 179 (17%) |
| Unknown | 132 |
| pT category | |
| 1 | 696 (57%) |
| 2 | 339 (28%) |
| 3 | 181 (15%) |
| TOLMS cordectomies according to the ELS (12,13) | |
| 1-2 | 419 (35%) |
| 3-6 | 789 (65%) |
| Unknown | 8 |
| Margin status | |
| Free/close | 772 (63%) |
| Positive | 444 (37%) |
| Postoperative management | |
| Follow-up (free/close margins) | 772 (63%) |
| Second-look surgery | 207 (17%) |
| Adjuvant therapy | 72 (5.9%) |
| Second-look surgery + adjuvant therapy | 15 (1.2%) |
| Surveillance (positive margins) | 150 (12%) |
| Residual carcinoma after second-look surgery | 61 (5%) |
| Follow-up time | 61 (33, 97) |
| Total laryngectomy | 64 (5.3%) |
| Last follow-up status | |
| NED | 970 (80%) |
| AWD | 9 (1%) |
| DOC | 176 (14%) |
| DOD | 61 (5%) |
| Data are presented as number (%) unless otherwise indicated. Continuous variables are reported as median (interquartile range). TOLMS, transoral laser microsurgery; ELS, European Laryngological Society ( 12 , 13 ); pT, pathologic tumour category; NED, no evidence of disease; AWD, alive with disease; DOC, death from other causes; DOD, death from disease. | |
| Margin status/main finding | Key message |
|---|---|
| Margin positivity (overall concept) | Margin positivity after TOLMS is not a binary prognostic variable. Oncologic risk is driven by margin type and burden (single superficial, multiple superficial, deep), rather than by a simple positive/negative classification |
| Single superficial positive margin | Behaves comparably to free margins in terms of DFS, supporting conservative postoperative management and surveillance in appropriately selected patients |
| Multiple superficial or deep margin involvement | Oncologic risk increases with margin burden. Multiple superficial margins are associated with a higher risk of recurrence, while deep margin involvement represents the most adverse pattern, independently associated with both recurrence and disease-specific mortality |
| Residual carcinoma at second-look surgery | Identifies a distinct high-risk subgroup with markedly worse DFS and DSS. Oncologic outcomes in these patients suggest aggressive tumour biology or failure of endoscopic disease control, supporting intensive surveillance, or early treatment escalation beyond endoscopic-only strategies |
References
- SEER Cancer Stat Facts: Larynx Cancer.
- Huang J, Chan S, Ko S. Updated disease distributions, risk factors, and trends of laryngeal cancer: a global analysis of cancer registries. Int J Surg. 2024;110:810-819. doi:https://doi.org/10.1097/JS9.0000000000000902
- Mousavi S, Ilaghi M, Aslani A. Laryngeal cancer incidence trends in the United States over 2000-2020: a population-based analysis. Arch Public Health. 2024;82. doi:https://doi.org/10.1186/s13690-024-01333-1
- Marchi F, Del Bon F, Chu F. Refining prognostic subcategories in intermediate-advanced glottic cancer: a multicentric study on 637 patients treated by transoral laser microsurgery. Oral Oncol. 2025;164. doi:https://doi.org/10.1016/j.oraloncology.2025.107264
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Head and Neck Cancers.
- Mannelli G, Meccariello G, Deganello A. Impact of low-thermal-injury devices on margin status in laryngeal cancer: an experimental ex vivo study. Oral Oncol. 2014;50:32-39. doi:https://doi.org/10.1016/j.oraloncology.2013.10.001
- De Virgilio A, Pagliuca G, Russo E. Prognostic significance of surgical margins in laryngeal cancer treated by transoral laser microsurgery: a systematic review and meta-analysis. Acta Otorhinolaryngol Ital. 2025;45:S71-S86. doi:https://doi.org/10.14639/0392-100X-suppl.1-45-2025-N1142
- Piazza C, Paderno A, Grazioli P. Laryngeal exposure and margin status in glottic cancer treated by transoral laser microsurgery. Laryngoscope. 2018;128:1146-1151. doi:https://doi.org/10.1002/lary.26861
- Peretti G, Piazza C, Cocco D. Transoral CO(2) laser treatment for T(is)-T(3) glottic cancer: the University of Brescia experience on 595 patients. Head Neck. 2010;32:977-983. doi:https://doi.org/10.1002/hed.21278
- Ansarin M, Cattaneo A, De Benedetto L. Retrospective analysis of factors influencing oncologic outcome in 590 patients with early-intermediate glottic cancer treated by transoral laser microsurgery. Head Neck. 2017;39:71-81. doi:https://doi.org/10.1002/hed.24534
- Mariani C, Carta F, Bontempi M. Management and oncologic outcomes of close and positive margins after transoral CO2 laser microsurgery for early glottic carcinoma. Cancers (Basel). 2023;15. doi:https://doi.org/10.3390/cancers15051490
- Blanch J, Vilaseca I, Bernal-Sprekelsen M. Prognostic significance of surgical margins in transoral CO2 laser microsurgery for T1-T4 pharyngo-laryngeal cancers. Eur Arch Otorhinolaryngol. 2007;264:1045-1051. doi:https://doi.org/10.1007/s00405-007-0320-2
- Ferrari M, Mularoni F, Smussi D. International consensus on laryngeal preservation strategies in laryngeal and hypopharyngeal cancer. Lancet Oncol. 2025;26:E264-E281. doi:https://doi.org/10.1016/S1470-2045(25)00020-8
- AJCC Cancer Staging System: Version 9. American College of Surgeons; 2024.
- Remacle M, Eckel H, Antonelli A. Endoscopic cordectomy. A proposal for a classification by the Working Committee, European Laryngological Society. Eur Arch Otorhinolaryngol. 2000;257:227-231. doi:https://doi.org/10.1007/s004050050228
- Remacle M, Van Haverbeke C, Eckel H. Proposal for revision of the European Laryngological Society classification of endoscopic cordectomies. Eur Arch Otorhinolaryngol. 2007;264:499-504. doi:https://doi.org/10.1007/s00405-007-0279-z
- Simo R, Bradley P, Chevalier D. European Laryngological Society: ELS recommendations for the follow-up of patients treated for laryngeal cancer. Eur Arch Otorhinolaryngol. 2014;271:2469-2479. doi:https://doi.org/10.1007/s00405-014-2966-x
- Piazza C, Filauro M, Paderno A. Three-dimensional map of isoprognostic zones in glottic cancer treated by transoral laser microsurgery as a unimodal treatment strategy. Front Oncol. 2018;8. doi:https://doi.org/10.3389/fonc.2018.00175
- Fiz I, Koelmel J, Sittel C. Nature and role of surgical margins in transoral laser microsurgery for early and intermediate glottic cancer. Curr Opin Otolaryngol Head Neck Surg. 2018;26:78-83. doi:https://doi.org/10.1097/MOO.0000000000000446
- Chu F, Bandi F, Pietrobon G. The real prognostic role of laryngeal dysplasia in patients affected by invasive cancer. Am J Otolaryngol. 2025;46. doi:https://doi.org/10.1016/j.amjoto.2024.104535
- Vander Poorten V, Meulemans J, Van Lierde C. Current indications for adjuvant treatment following transoral laser microsurgery of early and intermediate laryngeal cancer. Curr Opin Otolaryngol Head Neck Surg. 2021;29:79-85. doi:https://doi.org/10.1097/MOO.0000000000000702
- Iandelli A, Gabella G, Marchi F. The impact of margins in laryngeal cancer patients treated with transoral laser microsurgery: a systematic review and meta-analysis. Eur Arch Otorhinolaryngol. 2024;281:4485-4494. doi:https://doi.org/10.1007/s00405-024-08610-3
- Fiz I, Mazzola F, Fiz F. Impact of close and positive margins in transoral laser microsurgery for Tis-T2 glottic cancer. Front Oncol. 2017;7. doi:https://doi.org/10.3389/fonc.2017.00245
- Pinacoli A, Ruiz-Sevilla L, Sampieri C. Optimising oncologic outcomes in pT3 glottic cancers treated by transoral laser microsurgery: the impact of adjuvant treatment. Acta Otorhinolaryngol Ital. 2025;45:388-398. doi:https://doi.org/10.14639/0392-100X-A1372
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 351 times
- PDF downloaded - 120 times