Clinical techniques and technologies
Vol. 45: Issue 5 - October 2025
Technological refinements in transoral laser exoscopic surgery: the VITOM EAGLE
Summary
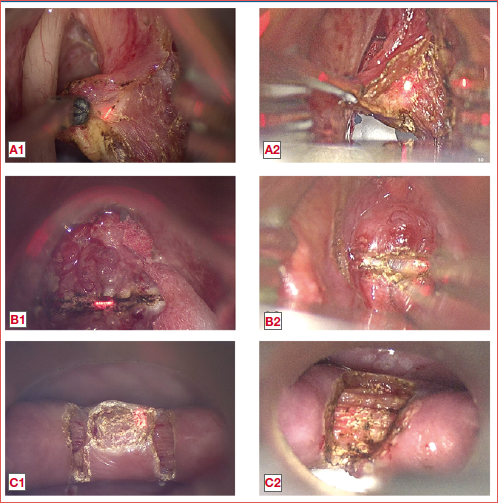
Cover Image
Traditionally, microscopes have been the primary magnification tools in head and neck surgery, offering excellent illumination, augmentation, and three-dimensional (3D) visualisation. More recently, exoscopes such as the VITOM 3D from Karl Storz, have emerged. These devices utilise high-definition cameras to project 3D views onto a screen, enabling the entire surgical team to observe the procedure while the first operator assumes a more ergonomic position during surgery. VITOM 3D enhances surgical accuracy and team collaboration, although it presents challenges including difficulties with focus at high magnification and less stable coupling with adjunctive tools. To address these limitations, the VITOM EAGLE exoscope was recently introduced. Weighing 4 kg, it features a 6X optical and 2X digital zoom, 4K resolution, stepless focus adjustment, and a 90° viewing angle. It offers improved ergonomics even compared to the previous VITOM 3D, better laser coupling stability, and enhanced visualisation capabilities, especially at higher magnification. The VITOM EAGLE’s controls include an IMAGE1 PILOT, footswitch, and head buttons, managing functions like focus, zoom, brightness, and image capture. Despite its advancements, some details, like the smoothness of the robotic arm, still require refinement. In our clinical practice, several cases were managed with the use of the VITOM 3D and, more recently, with VITOM EAGLE, some of which are illustrated herein.
Introduction
Traditionally, the microscope has been the primary tool for magnification in various subspecialties of head and neck surgery, providing excellent illumination and magnification but with suboptimal ergonomics and difficulty in sharing the visualisation of the surgical field with assistants and nurses 1. In the last decade, the exoscope has therefore emerged as a transformative technology that employs a high-definition camera to project a 3D view onto a wide screen, allowing the entire operating room staff to observe the procedure through polarised glasses 2,3.
Initially introduced to address significant drawbacks of microscopes, such as a restricted 3D vision exclusive to the primary operator, the VITOM 3D exoscope (Karl Storz – Tuttlingen, Germany), demonstrated other potential benefits 4,5. It enhances surgical visualisation and magnification, thereby improving surgical accuracy, better illumination and 3D perception even through small bored laryngoscopes, where the traditional microscopic view was mostly monocular. Moreover, it facilitates the use of multiple instruments and lasers simultaneously during procedures by a 3- or 4-hand technique, promoting successful outcomes without additional complications 6,7. Furthermore, it fosters better collaboration among the surgical team by enabling everyone to have a 3D view of the surgical field on wide monitors. However, daily use of VITOM 3D has revealed some intrinsic limitations, including challenges with focus at high magnification and less stable laser coupling.
As a progression in the exoscopic technology, the VITOM EAGLE (Karl Storz, Tuttlingen, Germany) was introduced in 2024 to potentially overcome these limitations. The advantages of the VITOM EAGLE are particularly significant in carbon dioxide transoral laser microsurgery (CO2 TOLMS)8 that should be, in this sense, here more appropriately termed transoral laser exoscopic surgery (CO2 TOLES), where the narrow and deep surgical field requires enhanced visualisation of small anatomical details, proper ergonomics, and sufficient illumination.
To date, no publications have reported on the use of the VITOM EAGLE in TOLMS. This article aims to present our clinical experience with the VITOM 3D and the newly introduced VITOM EAGLE, comparing the pros and cons, and highlighting how its technical improvements have turned into practicality in the field of head and neck surgery.
Description of the new technology
The VITOM EAGLE overview is illustrated in Figure 1, while its main technical characteristics, compared to those of VITOM 3D, are presented in Table I. The VITOM EAGLE weighs 4 kg and boasts a 6X optical zoom with an additional 2X digital zoom (totaling 12X). Control options are managed through the IMAGE1 PILOT, footswitch, and head buttons. It features seven illumination spots, operates at 4K resolution with four 4K sensors, offers stepless focus adjustment, and provides a 90° viewing angle. The image of the VITOM EAGLE can be rotated around its central axis, allowing for flexible positioning as well as correction of the horizontal orientation of the image during use.
Unlike the VITOM 3D, which is equipped solely with digital zoom, the VITOM EAGLE features both digital and optical zooms, facilitating seamless transition between the two. The functions of enlarging, reducing and focusing the image are managed through the IMAGE1 PILOT (Fig. 2). The foot pedal can be functionally coupled with it to manage the movements of the robotic arm. The focal distance can be continuously adjusted between approximately 20-50 cm.
The function buttons on the VITOM EAGLE are as follows:
- upper-level focus (short and long press);
- fluorescence on/off (short press), brightness setting (long press);
- image enlargement (short and long press);
- if the menu is active, back/close menu (short and long press);
- image reduction (short and long press);
- image capture (short press) and video recording (long press);
- lower-level focus (short and long press);
- open live menu (short press) and open setup menu (long press).
Image exposure can be adjusted using the diaphragm filter wheel to increase or decrease the light spot size, allowing for the use of laryngoscopes with narrower lumens by reducing light reflection on the laryngoscope walls. There are also several function buttons on the IMAGE1 PILOT, including: white balance, capture, light source intensity, video, brightness, RIP-Swap, and Kmage Glip.
In terms of ergonomics, the first operator using the VITOM EAGLE enjoys unobstructed vision directly towards the screen, without interference as was the case with the previous VITOM 3D arm, lying vertically between the surgeon and the screen (Fig. 3). Furthermore, the coupling with laser is significantly more stable.
The VITOM EAGLE has undergone significant technical improvements in terms of illumination. By reducing the number of lenses and elements in the optical path, it exhibits significantly higher light transmission compared to the VITOM 3D. The illumination in the VITOM EAGLE now occurs along the same optical axis used for observing the scene. This results in reduced shadowing and allows for much deeper illumination of narrow cavities and access points. In contrast, the illumination in the VITOM 3D was still offset at an angle next to the lenses. The effective use of the illuminated area is higher in the VITOM EAGLE, resulting in less wasted light.
Piazza et al. 6 previously emphasised the ergonomic benefits of the VITOM 3D compared to the conventional microscope, as evaluated through surface electromyography monitoring of the most involved muscular groups of the neck and shoulders. The VITOM EAGLE apparently further augments these advantages by offering the surgeon a completely unobstructed field of vision, as no parts of the equipment are positioned within the line of sight (Fig. 3). This could translate in reduced lateral bending of the neck and back with further gain in terms of reduced fatigue of the surgeon during long procedures.
Discussion
In our clinical practice, several cases have been managed with the use of the VITOM EAGLE, some of which are described below. Each pathology has been treated with the use of both VITOM EAGLE and VITOM 3D in different patients to underline the advantages of the VITOM EAGLE.
Case 1
A 76-year-old male presented with a one-year-long history of persistent dysphonia. He had a history of smoking (30 packs/year) and had never undergone previous laryngeal procedures. During clinical evaluation, videoendoscopy demonstrated a suspicious lesion involving the middle third of the right vocal cord with atypical vascular pattern at bioendoscopy and normal vocal cord mobility. A subligamental cordectomy (type II according to the European Laryngological Society [ELS] classification) 9 using the VITOM EAGLE was performed (Cover figure, A1). The histopathological examination confirmed the lesion to be a squamous cell carcinoma (SCC) with negative surgical margins. The patient underwent an uneventful postoperative hospitalisation and was discharged the day after surgery. The use of the VITOM EAGLE in this case enabled better focusing of the laser spot due to the reduction in laser beam size. This improvement results in less tissue carbonisation compared to cases treated with the VITOM 3D (Cover figure, A2), due to the ability to continuously maintain the laser beam well focused on the target throughout the entire procedure.
Moreover, in early stage glottic tumours, the goals of transoral laser surgery are to remove the disease and preserve vocal function, while adhering to the principles of a minimally-invasive phonosurgical approach. Therefore, maintaining the integrity of the vocal muscle during subligamental cordectomy is essential. The VITOM EAGLE, with its superior resolution at high magnification, allows for more detailed visualisation of the plane between the vocal ligament and the muscle, enabling a more precise, muscle-sparing dissection, which contributes to better preservation of vocal cord function.
Case 2
A 40-year-old man with a history of smoking (35 packs/year) presented with dysphonia. At videoendoscopy, a leukoerythroplasic lesion involving the left true vocal cord with extension to the ipsilateral false cord, involvement of the anterior commissure and initial supracommisural extension was visible. Computed tomography excluded pre-epiglottic and/or cartilaginous framework involvement. A cordectomy type V abcd according to the ELS with multiblock technique using the VITOM EAGLE (Cover figure, B1) was performed. The multiblock technique is usually employed to facilitate a more precise excision in cases of bulky lesions not fully visible in their subglottic, lateral or transcommissural extension without sequentially removing parts of the lesion itself. Due to the restricted operative field in which the procedure is conducted, excellent visualisation of the tumour is mandatory to provide adequate control of the surgical margins and bleeding. The lesion was confirmed to be a SCC, with depth of invasion of 4 mm, without lymphovascular and/or perineural invasion. All surgical margins were reported as clean. During a multiblock resection, it is often necessary to change the laryngoscope and/or its position, especially for management of the most anterior and posterior aspects of the tumour, thus achieving better exposure. Consequently, a more effective control of macroscopic margins can be obtained. To get precise and focused visualisation, it is frequently required to adjust the position of the exoscope itself. Therefore, the improved ergonomics and the precise collimation of the coupled laser micromanipulator are crucial in handling such cases. Furthermore, the VITOM EAGLE allows the use of laryngoscopes with narrower lumens by decreasing the diameter of the light beam spot, which in turn minimises reflection on the surfaces of the laryngoscope, and still maintaining a 3D vision, differently from what is commonly observed through a microscope which presents a larger inter-ocular distance. Overall, the features of the VITOM EAGLE enhance the management of these lesions compared to the VITOM 3D (Cover figure, B2)
Case 3
An 80-year-old female presented with complaints of dysphagia and regurgitation. She had a history of previous surgeries for intestinal diverticulosis and occlusion. Videoendoscopy demonstrated hypopharyngeal salivary pooling. A barium swallow test with videofluoroscopy was performed, showing a 20 x 25 mm Zenker’s diverticulum. Therefore, a CO2 TOLES diverticulotomy with VITOM EAGLE was performed, incising the cricopharyngeal muscle between the oesophageal lumen and the diverticulum pouch through a bivalved laryngoscope or diverticuloscope (Cover figure, C1). The patient experienced an uncomplicated postoperative hospitalisation and was discharged on the first postoperative day. The VITOM EAGLE, compared to the VITOM 3D (Cover figure, C2), delivers excellent views of detailed anatomical features, enhancing magnification by combining optical and digital zooms. This feature was particularly useful during diverticulotomy, allowing for precise visualisation of the incision of muscle fibres through the entire thickness of the cricopharyngeal muscle. The diverticuloscope is narrower and longer compared to any laryngoscope. Therefore, the VITOM EAGLE is highly useful in such a case, where the field’s luminosity is lower, and the depth of field is greater compared to a standard laryngoscope. While handling such cases, the improved focusing capabilities of VITOM EAGLE, compared to the VITOM 3D, enable better focus on deeper fields and allow for a reduction of the diameter of the light beam spot, thereby minimising light reflection within the narrow lumen of the diverticuloscope.
Case 4
This is a case of a 47-year-old female diagnosed with a right laryngeal paraganglioma. The patient is a carrier of an SDHB mutation and had a history of previous mediastinal paraganglioma resection. Videoendoscopy demonstrated a vascularised lesion at the level of the right arytenoid, with normal laryngeal motility. An endoscopic blanching procedure with TRUEblue laser (A.R.C. laser system) using the VITOM EAGLE was performed (Fig. 4A). As demonstrated in this case, the VITOM EAGLE shares with the VITOM 3D (Fig. 4B) the ability to use various surgical tools during surgery, such as the blue laser or other fibre lasers as demonstrated by Deganello et al. 10.
Case 5
An 85-year-old patient presented with a left internal laryngocele. Videoendoscopy identified the lesion as a left false cord bulging, without atypical vascular pattern. We performed a CO2 TOLES using the VITOM EAGLE. As clearly shown in Figure 5a, the VITOM EAGLE allows for the use of narrower laryngoscopes due to the decreased diameter of the light beam spot compared to the VITOM 3D (Fig. 5B), minimising the reflection of light on the inner walls of the laryngoscope and reducing shadowing, especially in narrow cavities and restricted access points.
Conclusions
VITOM EAGLE is a versatile tool designed to provide excellent visualisation of small anatomical details. It offers enhanced visualisation at higher magnification through the integration of optical and digital zooms, featuring better ergonomics compared to the VITOM 3D. Additionally, the fixed coupling with laser micromanipulator ensures precise collimation. The VITOM EAGLE also allows for the use of laryngoscopes with narrower lumens by reducing the diameter of the light beam spot, thereby reducing light reflection on the laryngoscope walls. To the best of our knowledge, these are the only cases reported in the literature demonstrating how the VITOM EAGLE embraces all the advantages of the microscope, while simultaneously overcoming the limitations of the previous VITOM 3D and the well-known drawbacks of the surgical microscope. However, a few details still require refinement, such as the manoeuvrability and smoothness of the robotic arm during minimal adjustments in surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
FM, MF, GP: study conception; MF, EB: study design; FM, MF, AP: data collection; FM, AP, EB: draft manuscript preparation. CP, GP: approved the final version of the manuscript.
Ethical consideration
This study was approved by the Institutional Ethics Committee (CER Liguria: 220/2024). The research was conducted ethically, with all study procedures being performed in accordance with the requirements of the World Medical Association’s Declaration of Helsinki.Written informed consent was obtained from each partici-pant/patient for study participation and data publication.
History
Received: December 29, 2024
Accepted: January 13, 2025
Figures and tables
Figure 1. Overview of the VITOM EAGLE. 1) Function button; 2) Activation button for manual operation; 3) Fiber optic cable; 4) Operative window; 5) Mounting for autostatic arm; 6) Network cable socket; 7) Video cable; 8) Diaphragm filter wheel.
Figure 2. Picture of the IMAGE1 PILOT. 1) Programmable buttons (1-4) for quick access; 2) ESC button; 3) ENTER button.
Figure 3. Ergonomic position adopted by the surgeon: left image using VITOM EAGLE, and right image with VITOM 3D. The use of the VITOM EAGLE allows an even better intraoperative position due to the unobstructed view of the surgical screen.
Figure 4. Endoscopic blanching procedure with TRUEblue laser (A.R.C. laser system) using the VITOM EAGLE (A). Endoscopic blanching procedure with TRUEblue laser (A.R.C. laser system) using the VITOM 3D (B).
Figure 5. Endoscopic resection of a left internal laryngocele with CO2 laser using the VITOM EAGLE (A). Endoscopic resection of a left internal laryngocele with CO2 laser using the VITOM 3D (B).
| VITOM® 3D | VITOM® Eagle | |
|---|---|---|
| Weight (camera) | 1 kg | 4 kg |
| Zoom | 4X digital | 6X optical + 2X digital (12X) |
| ROI available | Yes | Yes, only in digital zoom |
| Control options | IMAGE1 PILOT + foot pedal | IMAGE1 PILOT + foot pedal + head buttons |
| Illumination spots | No | Yes (7 spots) |
| Resolution | Full HD | 4K |
| Sensors | 2 x 4K | 4 x 4K |
| Focus | Stepless | Stepless |
| Angulation | 90° | 90° |
| Working distance | Approx. 20-50 cm | Approx. 20-50 cm |
References
- Carobbio A, Missale F, Fragale M. Transoral laser microsurgery: feasibility of a new exoscopic HD-3D system coupled with free beam or fiber laser. Lasers Med Sci. 2021;36:1865-1872. doi:https://doi.org/10.1007/s10103-020-03221-w
- Marchi F, Bellini E, Ioppi A. Enhancing quality of life in head and neck cancer patients: a comparative analysis of 3D exoscope-assisted surgery vs. traditional approaches. Front Surg. 2024;11. doi:https://doi.org/10.3389/fsurg.2024.1358500
- Shirzadi A, Mukherjee D, Drazin D. Use of the video telescope operating monitor (VITOM) as an alternative to the operating microscope in spine surgery. Spine. 2012;37:1517-1523. doi:https://doi.org/10.1097/BRS.0b013e3182709cef
- Ferlito S, La Mantia I, Caruso S. High definition three-dimensional exoscope (VITOM 3D) in ENT surgery: a systematic review of current experience. J Clin Med. 2022;11:1-20. doi:https://doi.org/10.3390/jcm11133639
- Paderno A, Deganello A, Lancini D. Is the exoscope ready to replace the operative microscope in transoral surgery?. Curr Opin Otolaryngol Head Neck Surg. 2022;30:79-86. doi:https://doi.org/10.1097/MOO.0000000000000794
- Piazza C, Gennarini F, Montenegro C. Transoral laser exoscopic surgery of the larynx: state of the art and comparison with traditional transoral laser microsurgery. Acta Otorhinolaryngol Ital. 2024;44:S3-S11. doi:https://doi.org/10.14639/0392-100X-suppl.1-44-2024-N2850
- Marchi F, Bellini E, Ioppi A. Maximising efficiency with exoscopic surgery: a versatile approach for transoral laryngeal and oropharyngeal procedures. Acta Otorhinolaryngol Ital. 2024;44:368-376. doi:https://doi.org/10.14639/0392-100X-N2958
- Remacle M, Arens C, Eldin M. Laser-assisted surgery of the upper aero-digestive tract: a clarification of nomenclature. Eur Arch Otorhinolaryngol. 2017;274:3723-3727. doi:https://doi.org/10.1007/s00405-017-4708-3
- Remacle M, Van Haverbeke C, Eckel H. Proposal for revision of the European Laryngological Society classification of endoscopic cordectomies. Eur Arch Otorhinolaryngol. 2007;264:499-504. doi:https://doi.org/10.1007/s00405-007-0279-z
- Deganello A, Gualtieri T, Testa G. Exoscopic transoral supraglottic laryngectomy. Laryngoscope. 2025;135:744-747. doi:https://doi.org/10.1002/lary.31767
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2025 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 1214 times
- PDF downloaded - 208 times