Annual congress report
Vol. 46: 112 TH CONGRESS SIOECHCF - OFFICIAL REPORT 2026
The neck matters: optimising lymph node management in laryngeal cancer
Authors
Pierre Guarino
 , Francesco Chiari
, Gerardo Petruzzi
, Francesco Mazzola
, Milena Fior
, Alessandro Borrelli
, Raul Pellini
, Giuseppe Spriano
, Filippo Ricciardiello
, Claudio Donadio Caporale
, Francesco Chiari
, Gerardo Petruzzi
, Francesco Mazzola
, Milena Fior
, Alessandro Borrelli
, Raul Pellini
, Giuseppe Spriano
, Filippo Ricciardiello
, Claudio Donadio Caporale
Summary
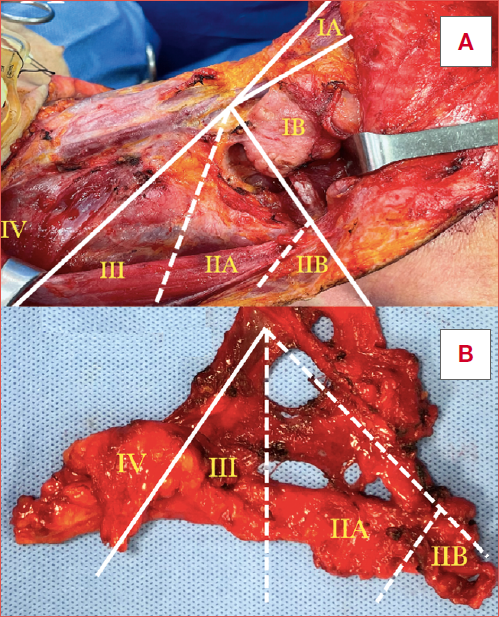
Cover Image
Objective. Laryngeal squamous cell carcinoma (LSCC) accounts for nearly one quarter of head and neck malignancies, with cervical nodal status representing the strongest prognostic factor. This review aims to summarise evidence on neck management across different clinical scenarios.
Methods. A narrative review of PubMed, Scopus, and Web of Science was conducted up to July 2025. Original studies, systematic reviews, meta-analyses, and clinical guidelines were included. Data were analysed according to clinical setting: cN0, cN+, rcN+, and rcN0.
Results. In primary cN0 LSCC, the risk of occult nodal disease is site-dependent. Supraglottic tumours show the highest incidence (20-50%, > 50% in T3-T4), supporting elective bilateral selective neck dissection (SND) of levels II-IV, with level VI in selected cases. Early glottic tumours rarely metastasise (< 10%) and may be observed, while advanced glottic and subglottic tumours show higher risk (15-30%), justifying elective treatment. In cN+ disease, SND is indicated for N1-N2 and modified radical neck dissection for N3. Regional recurrence occurs in 15-25% of cases. In rcN+ disease, salvage SND provides regional control comparable to comprehensive dissection with lower morbidity. The role of elective dissection in rcN0 remains controversial despite occult metastasis rates > 20% in high-risk tumours.
Conclusions. Neck management in LSCC should be adapted to risk: elective treatment is essential in high-risk cN0 disease, therapeutic dissection remains standard in cN+, and salvage SND is effective in rcN+, while elective treatment in rcN0 should be reserved for selected cases.
Introduction
Laryngeal squamous cell carcinoma (LSCC) accounts for approximately 20-25% of all head and neck cancers (HNC) and 1-2% of all malignancies worldwide, with an estimated global incidence of 2-5 cases per 100,000 population per year 1. The highest rates are reported in Europe and Northern America, reflecting the strong association with tobacco and alcohol consumption 2. In the United States and several European countries, the incidence has shown a gradual decline over recent decades, largely attributable to reduced tobacco use, though the disease still carries a significant global burden 2. On the other hand, the prognosis has not improved significantly, with a 5-year overall survival (OS) of 60.9% 3.
LSCC primarily affects men, with male-to-female ratio ranging between 4:1 and 8:1. Peak incidence occurs in the sixth to seventh decade of life, although increasing numbers of younger adults have been reported 4. Globally, LSCC remains a major health concern with 100,000 deaths reported in 2022. While mortality rates have decreased on a population-adjusted basis, the aging and growth of the global population have resulted in rising absolute numbers, reinforcing the importance of effective staging and management of cervical disease 5.
The primary tumour subsite strongly influences the risk and pattern of cervical nodal metastasis. Supraglottic carcinomas, which represent 30-40% of LSCC, are characterised by abundant lymphatic drainage and frequent bilateral spread to levels II-IV. Consequently, clinically positive lymph nodes are observed in 40-60% of patients at diagnosis, and bilateral involvement has been reported in up to 20% of cases. Even in clinically N0 (cN0) supraglottic tumours, occult metastases may exceed 50%, particularly in advanced T categories 6. By contrast, glottic tumours have limited lymphatic drainage and are globally associated with nodal disease in only 10-20% of cases, most often in advanced T categories (T3-T4), where the risk of occult metastasis may rise to 15-30% 7. Subglottic tumours exhibit intermediate risk, with nodal involvement ranging between 20-50% at diagnosis, typically involving pre-laryngeal, paratracheal, and lower cervical nodes 7.
Management of the neck in LSCC is one of the most critical determinants of prognosis. The complexity arises from the heterogeneity of LSCC: supraglottic tumours carry a high risk of occult nodal metastases warranting elective treatment, while early glottic cancers rarely spread to cervical nodes, making the need for prophylactic intervention debated 8.
The aim of this narrative review is to provide an updated synthesis of current strategies for neck management in LSCC, with particular emphasis on the prognostic impact of nodal status and its implications for surgical decision-making in both cN0 and cN+ disease, as well as in recurrent disease.
Materials and methods
This narrative review was conducted to summarise and critically discuss current evidence on neck management in LSCC. A comprehensive literature search was performed in PubMed/MEDLINE, Scopus, and Web of Science from January 2000 to July 2025, using combinations of the following keywords: laryngeal cancer, laryngeal squamous cell carcinoma, neck dissection, neck management, nodal metastasis, elective neck dissection, elective neck irradiation, lymph node ratio, and extranodal extension.
Original research articles, systematic reviews, meta-analyses, and relevant guidelines published in English were considered. Case reports or series, conference abstracts, and articles not directly addressing the management of the neck in LSCC were excluded. Priority was given to high-quality studies, landmark articles, and recent publications providing novel insights into patterns of lymphatic spread, diagnostic strategies, and therapeutic approaches.
Several types of neck dissection have been described in the literature, differing in extent and functional morbidity. For this review, all procedures reported in the studies analysed were considered, including radical (RND), modified radical (mRND), elective (END), selective (SND), and, when applicable, super-selective neck dissections (SSND), according to the definitions provided by the original authors.
The review was organised thematically, focusing on: (1) management of cN0 neck, (2) management cN+ neck, (3) management of rcN+ neck, and (4) management of rcN0 neck. Given the narrative nature of this review, no formal quality assessment or meta-analysis was performed.
Results
The main findings of this narrative review are summarised in Tables I-III. The tables describe patterns of lymphatic spread, risk of occult nodal metastases, and surgical indications for neck dissection according to primary laryngeal subsite and clinical nodal status (cN0, cN+, rcN+, and rcN0).
Discussion
The role of neck dissection in the cN0 setting
Optimal management of the cN0 scenario in LSCC remains one of the most debated issues in head and neck oncology. While nodal metastasis is the most important prognostic determinant, the risk of occult disease varies substantially according to tumour subsite, TNM staging, and clinical features. Decisions regarding neck dissection must therefore balance the oncologic risk of undertreatment with the functional morbidity of unnecessary intervention. Table I compares different neck dissection strategies in LSCC highlighting subsite-related patterns of lymphatic spread and tailored indications. In supraglottic carcinoma, the risk of occult nodal metastasis is particularly high, ranging from 20 to 50% in clinically cN0 patients and exceeding 50% in advanced cT3-T4 tumours 1. This is attributable to the rich lymphatic network of the supraglottis, which drains bilaterally into multiple cervical levels, predominantly levels II, III, and IV, with occasional involvement of level V 8. Sanabria et al. 7 demonstrated that among cervical lymph nodes levels, levels II and III are the most frequently involved in supraglottic LSCC, representing the principal sites of occult nodal spread. By contrast, the risk of metastasis in other levels is considerably lower. Specifically, occult involvement of level I has been reported in 2.4% of cases, level IV in 2%, level V in 0.4%, and sublevel IIb in 0.5%7. Furthermore, Ma et al. 9, in a retrospective study of cN0 supraglottic LSCC patients, reported occult metastases in 19.6% of level II nodes, 17.2% of level III, and only 3.6% of level IV. Similarly, Xu et al.10 described ipsilateral occult disease rates of 21% at level II, 11.1% at level III, and 1.6% at level IV. Bilateral nodal disease has been documented in 10-20% of cases, further supporting the need for comprehensive management with bilateral neck treatment. More recent studies confirm the clinical relevance of contralateral involvement. Hut et al. 11 reported bilateral nodal metastases at diagnosis in approximately 16% of patients, while Xu et al. 10 observed contralateral occult metastases in 6-7% of cases (levels II-III), with an overall occult metastasis rate of 35%. Conversely, Gatti et al. 12 demonstrated that in patients with cN0 contralateral neck, the risk of occult disease is < 20%, suggesting that routine bilateral neck dissection may not always be warranted. Wen et al. 13 recently reported, in a meta-analysis including 1,609 patients with cN0 supraglottic LSCC, an overall rate of occult contralateral metastases of 7.5%. The risk varies from 4.1% in lateralised tumours to 13.6% in those crossing the midline. Bilateral or contralateral neck dissection is therefore recommended only for lesions involving the midline or arising from subsites with rich contralateral lymphatic drainage, such as the epiglottis, the aryepiglottic fold, and the false vocal cord. Moreover, several studies confirmed that lymph nodes metastases at level IIb and IV are uncommon in cN0 supraglottic LSCC, with reported incidences of 0-2% at level IIb and 0-3.4% at level IV 14. A SSND has been explored in selected cases; however, despite the predictable lymphatic spread predominantly to levels II and III, it is not currently considered a standard approach 4.
In glottic LSCC, the risk of occult nodal spread is substantially lower, reflecting the relatively sparse lymphatic drainage of the true vocal cords. For early-T1-T2 lesions, the incidence of nodal metastasis is consistently < 5-10%, supporting a strategy of observation of the cN0 neck 15. Patel et al. 16, however, reported that higher tumour histopathologic grade was significantly associated with occult metastasis even in early glottic LSCC (p = 0.004). While END did not independently impact survival in their series, patients with occult nodal disease had significantly poorer outcomes (p < 0.001). In advanced glottic tumours (T3-T4), particularly those with anterior commissure or subglottic extension, the risk of occult metastasis increases substantially (15-30%), and END is therefore recommended 16. The meta-analysis by Sanabria et al. 7, including more than 3,800 patients, reported an overall rate of occult metastases of 8% (95% confidence interval, 2.7-13.3), compared with nearly 20% in supraglottic disease. Moreover, Sanabria et al. 7 reported that T1-T2 glottic LSCC rarely develop occult nodal spread (0-3%), while in advanced T3-T4 tumours the risk increases up to 15-20%, particularly involving levels II and III. Contralateral nodal involvement is uncommon (< 5%), and is generally restricted to transglottic tumours or those with anterior or posterior commissural extension. In conclusion, SSND is not considered standard in glottic cN0 tumours, as there is no robust evidence to guarantee oncologic safety.
The rare entity of subglottic carcinomas shows an intermediate risk of occult metastasis, estimated at 20-30% 17. Their lymphatic drainage differs from other subsites, involving the pre-laryngeal, pre-tracheal, and paratracheal nodes, as well as the lower jugular chain or mediastinum 9. These nodal groups are not consistently addressed by standard SND (levels II-IV). Consequently, in advanced subglottic tumours, elective treatment should be extended to include level VI (central compartment), either surgically or through elective nodal irradiation 5,9. Neglecting these nodes may predispose patients to isolated central recurrences, which are notoriously difficult to salvage. SSND is not regarded as an appropriate strategy, as limiting the dissection to fewer than 3 levels risks leaving occult disease untreated. Table II summarises the characteristics and indications for neck dissection based on the primary site of LSCC in cN0 neck.
In recent decades minimally-invasive surgical approaches, including transoral laser microsurgery (TOLMS) and transoral robotic surgery (TORS), have increasingly been adopted as part of organ-preservation strategies in selected LSCC 18-21. These approaches offer clear advantages in terms of laryngeal function, swallowing outcomes, and shorter recovery. One of the most debated aspects is that organ-preservation protocols often omit END in cN0 patients 22. While this avoids the morbidity of neck surgery, it carries the risk of leaving occult nodal disease untreated, particularly in supraglottic or advanced glottic tumours where the incidence of microscopic metastasis may exceed 20%. Several authors argue that combining minimally-invasive surgery of the primary tumour with END provides both functional preservation and accurate pathological staging, optimising the balance between oncologic safety and quality of life 23. However, the type of primary treatment should not influence management of the neck. The decision to perform END or irradiation should be guided by the T category and the estimated risk of occult nodal metastasis rather than by whether the primary tumour is treated surgically or through organ-preservation protocols.
The role of neck dissection in the cN+ setting
The presence of clinically positive lymph nodes (cN+) in LSCC profoundly influences both prognosis and the treatment strategy. Cervical nodal metastasis is associated with a 2- to 3-fold reduction in OS and significantly increases the risk of locoregional recurrence 24. According to the latest version of the National Comprehensive Cancer Network (NCCN, Ver. 5.5. 2025) Guidelines and the European Society for Medical Oncology (ESMO) Clinical Practice Guidelines, patients undergoing primary surgical treatment of the larynx should receive synchronous neck dissection, whereas those managed with definitive chemoradiation (CRT) should undergo therapeutic nodal irradiation, with appropriate fractionated dose 3,25. The standard surgical approach has traditionally been a SND or mRND, designed to ensure complete removal of metastatic disease. The extent of dissection is determined by the tumour subsite, the nodal burden (single vs multiple nodes, small vs bulky disease), and laterality (unilateral vs bilateral involvement) 26.
Specifically, clinical nodal metastases of supraglottic LSCC typically involve levels II-IV, with occasional spread to level V. The ESMO guidelines4 recommend therapeutic dissection of levels II-IV, extending to level V in cases of bulky or multilevel disease, N3, and bilateral dissection when contralateral nodes are suspicious 3. In supraglottic carcinoma with cN+ neck, the risk of contralateral nodal involvement is clinically relevant. Several studies have reported that the overall incidence of contralateral metastases ranges between 16 and 20%. Hut et al. 11 described bilateral nodal metastases in 16% of patients at diagnosis, while Xu et al. 10 observed occult contralateral metastases in 6-7% of cases, predominantly involving levels II and III. By contrast, contralateral involvement of level IV is very uncommon (< 1-2%), and metastases in levels I and V are virtually absent. These findings emphasise that in cN+ supraglottic carcinoma, contralateral nodal spread most often affects levels II and III, supporting the rational for contralateral END in patients with ipsilateral nodal disease.
In glottic carcinoma with clinically cN+ neck, the overall incidence of contralateral nodal metastases is generally low. In pure glottic tumours, contralateral involvement is rare, occurring in < 5% of cases. However, the risk increases to 10-15% in transglottic tumours or in those with subglottic extension or anterior/posterior commissure involvement 17. When present, contralateral nodal disease most frequently affects levels II and III, whereas contralateral metastases at level IV are very uncommon, and involvement of levels I and V is virtually absent. In purely glottic carcinomas, the risk of central neck compartment (CNC) metastases is low 27. However, when the tumour is advanced with subglottic extension, the likelihood of CNC involvement becomes clinically relevant (≈15-20%) 26. If the tumour is associated with subglottic or extra-laryngeal spread, the risk of CNC metastases becomes clinically relevant, and dissection should be considered. Conversely, if the disease remains strictly confined to the glottis without subglottic involvement, the probability of CNC metastases is very low, and elective dissection is not routinely recommended.
In subglottic carcinoma, nodal spread often involves levels III-IV as well as the central compartment (level VI). Both NCCN (Ver. 5.5. 2025) and ESMO guidelines recommend including levels II-IV plus level VI in the therapeutic dissection to prevent central compartment recurrence 3,25. Lucioni et al. 28 reported that CNC metastases occur in approximately 25-30% of subglottic LSCC, most frequently in association with extra-laryngeal extension or a history of preoperative tracheostomy. Similarly, Chabrillac et al. 29 in a recent meta-analysis confirmed a significantly increased risk of CNC involvement in T4 tumours with subglottic or extra-laryngeal spread. Importantly, Timon et al. 30 demonstrated that CNC metastases may occasionally represent the first echelon of lymphatic dissemination, arising even in the absence of lateral neck disease. Table III summarises the characteristics and indications for neck dissection based on the primary site of LSCC in cN+ neck.
Nodal status represents the most relevant prognostic determinant in LSCC, significantly influencing both treatment planning and oncological outcomes. According to the Eighth Edition of the TNM Staging System 31, N category is defined on the basis of the size, number, laterality, and extranodal extension (ENE) of metastatic lymph nodes, with staging ranging from N0 (absence of nodal disease) to N3 (node > 6 cm and/or ENE-positive). This classification is not merely descriptive, but has a direct impact on therapeutic decision-making. For early nodal involvement (N1), treatment may include SND alone, possibly followed by adjuvant radiation (RT) depending on additional risk factors such as perineural (PNI) or lympho-vascular invasion (LVI). In contrast, patients with advanced nodal disease (N2-N3) almost invariably require a multimodal approach, which often combines surgery, frequently a mRND approach, with adjuvant RT or concurrent CRT. Consequently, patients with multiple metastatic lymph nodes have significantly worse outcomes compared with those harbouring a single positive node 32. Particular emphasis is placed on the detection of ENE, which is recognized as an independent negative prognostic factor associated with markedly increased risk of locoregional recurrence and decreased OS 26,32. In this context, NCCN Guidelines (Ver. 5.5. 2025) strongly recommend postoperative CRT (generally with high-dose cisplatin) for patients with ENE or multiple involved nodes, as RT alone has been shown to be insufficient in this high-risk subgroup 4.
More recently, the lymph node ratio (LNR) has emerged as an independent prognosticator. High LNR has been linked to inferior OS and disease-specific survival (DSS) in LSCC, with proposed cutoff values ranging from 0.03 to 0.14 33. The pathological confirmation of these risk factors further strongly supports the need for adjuvant RT or concurrent adjuvant CRT 26,33. In parallel, the lymph node yield (LNY), representing the absolute number of nodes retrieved during dissection, has also been identified as a significant prognostic factor. A systematic review and meta-analysis by Iocca et al. 34 confirmed that both LNR and LNY correlate with survival outcomes in HNSCC, highlighting their potential to complement conventional nodal staging. These parameters not only reflect the biological aggressiveness of the disease but also provide a surrogate measure of surgical quality, further supporting their integration into risk stratification and adjuvant treatment planning.
While the therapeutic approach is largely dictated by nodal status and NCCN recommendations, the choice of surgical strategy must also carefully balance oncological radicality with functional preservation 4. In this context, SND has routinely been considered as a widely accepted procedure in patients with LSCC, as it provides adequate regional control while reducing morbidity compared with more extensive procedures. Compared with more radical procedures, SND offers reduced morbidity, particularly in relation to shoulder dysfunction, spinal accessory nerve injury, and cosmetic sequelae. Nevertheless, specific complications must be considered. The main risks associated with SND of levels II-IV include shoulder dysfunction due to manipulation of the spinal accessory nerve at level IIb, as well as potential injury to the phrenic nerve or thoracic duct at level IV. Even with nerve-sparing techniques, normal shoulder function is not always fully restored: only 70-75% of patients report complete recovery without impairment 35. Injury to the deep cervical plexus or the phrenic nerve can result in diaphragmatic paralysis, with reported rates ranging from 2.7% to 8% 36. Additionally, although rare, a chylous fistula may occur, with an incidence of approximately 5.5-5.8% 37. These findings underscore the importance of meticulous surgical technique and careful identification of critical anatomical structures and their anatomical variants, particularly during dissection of levels II-IV 38,39.
The role of neck dissection in the rcN+ setting
Regional recurrence following primary treatment of LSCC represents a major therapeutic challenge. Despite advances in multimodal management, 15-25% of patients develop nodal recurrence after initial therapy, and prognosis in this setting is generally poor, with 5-year OS rates ranging from 10 to 30% 40. There are 2 possible scenarios: recurrence after surgical treatment and recurrence after conservative treatment (RT/CRT). In particular, following (C)RT, 25-36% of advanced LSCC patients will need surgical salvage 41. Outcomes are strongly influenced by the timing of recurrence, extent of nodal disease, presence of ENE, and feasibility of salvage therapy. In the setting of recurrent or persistent nodal disease in LSCC, which the NCCN classifies under the category of “very advanced head and neck cancer”, therapeutic decision-making is primarily determined by the resectability and prior treatment history 4. In patients with surgically resectable nodal recurrence, salvage neck dissection is the treatment of choice. The indication for postoperative adjuvant therapy is based on clinical history, adverse pathological features, including ENE, positive surgical margins, and multiple nodal involvement, which represent well-established high-risk factors for locoregional failure and poor survival. In such cases, adjuvant CRT (typically cisplatin-based) is recommended, whereas RT alone or stereotactic RT may be considered in selected patients with contraindications to systemic therapy 42.
For patients with unresectable nodal recurrence who have not previously undergone neck irradiation, definitive RT with concurrent systemic therapy constitutes the standard of care, providing adequate performance status and organ function. This approach aims to achieve locoregional control while preserving quality of life, although long-term disease control rates remain limited in this subset. Moreover, in cases where patients are not candidates for curative surgery or re-irradiation due to prior treatment, management should shift toward immunotherapy (pembrolizumab), if adequate PD-L1 was seen 43.
Historically, salvage neck dissection consisted of mRND involving levels I-V, which was considered the standard treatment. However, most nodal recurrences involve levels II-IV, making mRND potentially an overtreatment associated with increased morbidity (i.e., spinal accessory nerve dysfunction, shoulder stiffness, and wound complications). Moreover, salvage neck dissection is technically demanding due to radiation-induced fibrosis, distorted anatomy, and impaired tissue vascularity, all of which contribute to higher complication rates compared with primary neck dissection. Reported morbidities include wound breakdown, pharyngocutaneous fistula, chyle leak, carotid artery exposure or rupture, and cranial nerve injury 40. Even when technically successful, functional sequelae such as shoulder dysfunction, dysphagia, and chronic pain are common, highlighting the importance of a careful risk-benefit assessment before considering salvage surgery. Several studies suggest that salvage SND is adequate in most rcN+ cases. In one series of 29 salvage neck dissections, 94% of viable metastases were confined to levels II-IV, with only one case involving level V 44. Another study of 68 neck dissections performed after CRT found that 98% of metastases were located at levels II-IV, and in 88% of cases they recurred in the same levels initially involved. Outcomes for SND and mRND were comparable, with slightly better OS observed in the SND group 45. A third study of 32 patients with isolated nodal persistence following CRT also demonstrated the efficacy of SND, with no new isolated nodal recurrences reported 46. There is also growing evidence supporting the use of SSND, targeting only one or two levels, in appropriately selected patients. Robbins et al. reported that in patients with residual disease confined to a single level, SSND (levels II-III) achieved excellent regional control (100%) compared with SND (91%) and mRND (82%) 47,48. In a pooled analysis of 35 SSNDs, no patients developed isolated nodal recurrences, further confirming its feasibility and effectiveness when residual disease is limited 49.
The role of neck dissection in the rcN0 setting
While therapeutic neck dissection is mandatory if feasible in patients with nodal recurrence, the role of neck dissection in rcN0 cases remains a matter of debate, particularly given its association with increased complication rates, such as wound breakdown and pharyngocutaneous fistula formation. A meta-analysis by Lin et al. 50 reported in a series of rT+ rN0 patients an overall occult nodal metastasis rate of 14%, which is below the classic 20% threshold proposed by Weiss et al. 51 as justification for SND. However, subgroup analyses revealed a significantly higher risk in supraglottic (24%), transglottic (17%), and advanced rT3-T4 recurrences, where several studies reported occult nodal metastasis rates exceeding 20%, and in some series reaching as high as 60%. Importantly, only Hilly et al. 52 showed a survival advantage with END, specifically in patients with rT3-T4 tumours, reporting markedly improved DFS and OS in this subgroup. In contrast, the majority of other studies failed to demonstrate significant differences in DFS or OS between SND and observation, findings that may reflect selection bias, small sample sizes, and heterogeneity in tumour subsites.
Taken together, these data suggest that END may be justifiable in selected high-risk groups – such as those with supraglottic or transglottic recurrences, and in patients with recurrent T3-T4 disease – where the risk of occult metastases exceeds the traditional threshold. However, its routine use in all salvage laryngectomy patients with rN0 necks is not supported by current evidence. Future well-designed, prospective studies are needed to clarify whether END confers a true survival benefit and to better define which patients may derive the greatest oncologic advantage from this intervention.
Future perspectives
Future research is increasingly focusing on the integration of biological and molecular markers into clinical decision-making. For example, the tumour microenvironment has emerged as a promising field of investigation. Recent multicentre initiatives, such as the protocol proposed by De Luca et al. 53, aim to evaluate the prognostic significance of stromal and immune-related features in LSCC. Incorporating such biomarkers may improve risk stratification and help identify patients who could benefit from tailored therapeutic intensification or, conversely, treatment de-escalation.
Moreover, the advent of liquid biopsy, particularly through detection of circulating tumour DNA (ctDNA), offers a minimally-invasive strategy that may significantly refine regional risk assessment in LSCC 54. In the context of cN0 LSCC, in fact, ctDNA may enable dynamic risk stratification. High pre- or postoperative ctDNA detection might signal elevated risk of occult nodal metastases, potentially prompting END. Moreover, serial ctDNA monitoring after primary treatment or in the recurrent setting may reveal molecular relapse or regional involvement before radiological or clinical signs arise, guiding timely surgical intervention or further diagnostic workup 55.
Beyond conventional imaging modalities, artificial intelligence and radiomics are emerging as promising tools for predicting occult nodal disease. A recent multicentre diagnostic study compared 3- and 2-dimensional deep-learning, radiomic, and fusion models based on computed tomography imaging in patients with LSCC, demonstrating that advanced computational models significantly improve the prediction of occult lymph node metastasis compared with standard imaging criteria 56. Such approaches may represent a paradigm shift in preoperative risk stratification, potentially guiding the indication for END in cN0 patients or define adjuvant therapeutic strategies 57.
Finally, standardisation of pathological assessment represents an additional key area for future development. Recent national data from Filippini et al. 58 highlight persistent diagnostic variability even among high-volume centres, underscoring the need for more uniform pathology workflows and structured reporting across head and neck oncology. Such variability likely affects the evaluation of critical prognostic features in LSCC – including ENE, LNR, and central compartment involvement – suggesting that improvements in pathological standardisation may directly enhance the accuracy of risk stratification and guide more individualised neck management strategies.
Conclusions
The management of the neck in LSCC must be tailored to nodal status at presentation and recurrence. In cN0 disease, the decision to perform END depends on subsite and T category. Elective treatment of the neck is essential in supraglottic and advanced glottic tumours, while in early glottic lesions clinical observation may be safely performed. In cN+ disease, SND or mRND remain the standard of care, with the extent determined by tumour location, nodal burden, ENE, and LNR. In the recurrent setting, neck management poses even greater challenges. For rcN+ disease, salvage SND or SSND may achieve satisfactory oncologic outcomes while reducing morbidity compared to more radical procedures, although surgery remains technically demanding in previously irradiated fields. In contrast, the role of END in rcN0 patients is still controversial: while supraglottic, transglottic, and advanced recurrent tumours may justify END due to higher rates of occult metastases, routine dissection is not supported by current evidence. Overall, these considerations highlight the need for a risk-adapted approach, integrating tumour subsite, stage, and pathological risk factors to optimise both oncologic safety and functional outcomes.
Acknowledgments
Francesco Mazzola is recipient of the Tor Vergata PhD program in Tissue Engineering and Remodelling Biotechnologies for Body Functions.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethical consideration
Not applicable.
History
Received: January 20, 2026
Accepted: March 21, 2026
Figures and tables
| Type | Levels involved | Structures removed | Supraglottic tumours | Glottic tumours | Subglottic tumours |
|---|---|---|---|---|---|
| RND | I-V | SCM, IJV, SAN | ENE+, N3 involving removed structures | ENE+, N3 involving removed structures | ENE+, N3 involving removed structure |
| mRND | I-V | Preserves ≥ 1 of SCM, IJV, SAN | N3, ENE+ with bulky multilevel nodes | N3, ENE+, with bulky disease | N3, ENE+, with bulky disease |
| SND | II-IV (± VI) | Preserves SCM, IJV, SAN | Standard in cN0 and cN+ (N1-N2b) (levels II-IV most at risk) | For locally advanced (cT3-T4) or subglottic extension (II-IV) and cN+ | For cN0 or cN+, II-IV + VI due to central compartment drainage |
| SSND | < 3 contiguous levels (e.g., II-III, III-IV) | Preserves all non-lymphatic structures | Salvage setting | Salvage setting | Salvage setting |
| ENE: extranodal extension; IJV: internal jugular vein; mRND: modified radical neck dissection; N: nodal status; RND: radical neck dissection; SAN: spinal accessory nerve; SCM: sternocleidomastoid muscle; SND: selective neck dissection; SSND: super-selective neck dissection. | |||||
| Subsite | Overall risk of occult metastasis | Most frequently involved levels | Reported incidence by level | Contralateral involvement | Treatment in cN0 neck |
|---|---|---|---|---|---|
| Supraglottic | 20-50% (up to > 50% in T3-T4) | II, III (± IV, rare V) | I: 2.4% | Levels II-III: 6-7% | END should always include levels II-III, often bilaterally |
| II: 19.6-21% | Overall bilateral: 10-20% | Level I and V are often omitted | |||
| IIB: 0-2% | |||||
| III: 11-17% | |||||
| IV: 1.6-3.6% | |||||
| V: 0.4% | |||||
| Glottic | 8% overall | II, III | II-III: 0-3% (T1-T2), 15-20% (T3-T4) | Rare (< 5%), usually transglottic or with commissural extension | Observation of cN0 neck standard in early tumors |
| < 5% in T1-T2 | END II-IV indicated in advanced disease | ||||
| 15-30% in T3-T4 | |||||
| Subglottic | 20-30% | II-IV, VI (pre-laryngeal, pre-tracheal, paratracheal) | IV: lower | Rare | Requires extension of elective treatment to include level VI |
| VI: up to 30% | |||||
| END: elective nodal dissection. | |||||
| Subsite | Levels involved | Contralateral metastasis risk | CNC (level VI) involvement | Treatment in cN+ neck |
|---|---|---|---|---|
| Supraglottic | II-IV (± V in bulky/multilevel disease) | Overall: 16-20%. (most often levels II-III) | Rare | Dissection of levels II-IV |
| Level IV < 1-2% | Extend to V in bulky/multilevel/ENE disease | |||
| Levels I and V virtually absent | Bilateral SND if contralateral nodes are suspicious | |||
| Glottic | II-III (advanced T categories) | Overall: < 5%, most commonly II-III | Low in pure glottic tumours | END is not routine in pure glottic tumours |
| Increases to 10-15% in transglottic tumours, with subglottic extension or commissure involvement | ≈15-20% if subglottic or extra-laryngeal extension or anterior commissure involvement | Consider CNC dissection if T3-T4 with subglottic/extra-laryngeal spread | ||
| Subglottic | III-IV + central compartment (level VI) | Not well defined | Frequent (20-30%) | Dissection of levels II-IV + VI |
| Contralateral uncommon | ||||
| CNC: central nodal compartment; SND: selective neck dissection. | ||||
References
- Ferlito A, Haigentz M, Bradley P. Causes of death of patients with laryngeal cancer. Eur Arch Otorhinolaryngol. 2014;271:425-434. doi:https://doi.org/10.1007/s00405-013-2478-0
- Steuer C, El-Deiry M, Parks J. An update on larynx cancer. CA Cancer J Clin. 2017;67:31-50. doi:https://doi.org/10.3322/caac.21386
- Hoffman H, Porter K, Karnell L. Laryngeal cancer in the United States: changes in demographics, patterns of care, and survival. Laryngoscope. 2006;116:1-13. doi:https://doi.org/10.1097/01.mlg.0000236095.97947.264
- NCCN Clinical Practice Guidelines in Oncology: Head and Neck Cancers. Version 5.2025.
- Jiang J, Xia Z, Yao W. Global, regional, and national larynx cancer burden and health inequality analysis from 1990 to 2021 with a prediction from 2022 to 2040. Front Oncol. 2025;15. doi:https://doi.org/10.3389/fonc.2025.1617613
- Kürten C, Zioga E, Gauler T. Patterns of cervical lymph node metastasis in supraglottic laryngeal cancer and therapeutic implications of surgical staging of the neck. Eur Arch Otorhinolaryngol. 2021;278:5021-5027. doi:https://doi.org/10.1007/s00405-021-06753-1
- Sanabria A, Shah J, Medina J. Incidence of occult lymph node metastasis in primary larynx squamous cell carcinoma, by subsite, T classification and neck level: a systematic review. Cancers (Basel). 2020;12. doi:https://doi.org/10.3390/cancers12041059
- Robbins K, Clayman G, Levine P. Neck dissection classification update: revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology-Head and Neck Surgery. Arch Otolaryngol Head Neck Surg. 2002;128:751-758. doi:https://doi.org/10.1001/archotol.128.7.751
- Ma H, Lian M, Feng L. Factors contributing to lymph node occult metastasis in supraglottic laryngeal carcinoma cT2-T4N0M0 and metastasis predictive equation. Chin J Cancer Res. 2014;26:685-691. doi:https://doi.org/10.3978/j.issn.1000-9604.2014.12.06
- Xu Y, Zhang Y, Xu Z. Patterns of cervical lymph node metastasis in locally advanced supraglottic squamous cell carcinoma: implications for neck CTV delineation. Front Oncol. 2020;10. doi:https://doi.org/10.3389/fonc.2020.01596
- Hut H, Remmelts A, de Keizer B. Prognostic significance of lymph node involvement in supraglottic laryngeal cancer: a retrospective cohort study. J Clin Med. 2025;14. doi:https://doi.org/10.3390/jcm1410336
- Gatti G, Giordano L, Bussi M. Management of the contralateral clinically negative neck in laryngeal squamous cell carcinoma: a review of current evidence. Braz J Otorhinolaryngol. 2025;9:155-163. doi:https://doi.org/10.1016/j.bjorl.2025.01.005
- Wen J, Liu C, Pan M. Bilateral neck dissection in cN0 supraglottic squamous cell carcinoma: essential or not?. Head Neck. 2025;47:2431-2438. doi:https://doi.org/10.1002/hed.28140
- Bassani S, Papi G, Marani F. Oncological feasibility of limited neck dissection in cN0 supraglottic laryngeal cancer. Head Neck. 2025;47:1699-1705. doi:https://doi.org/10.1002/hed.28081
- Rodrigo J, Silver C, Rinaldo A. Management of the clinically negative neck in early-stage glottic carcinoma. Eur Arch Otorhinolaryngol. 2017;274:2703-2709. doi:https://doi.org/10.1007/s00405-017-4507-2
- Patel T, Eggerstedt M, Toor J. Occult lymph node metastasis in early-stage glottic cancer in the National Cancer Database. Laryngoscope. 2021;131:E1139-E1146. doi:https://doi.org/10.1002/lary.28995
- Coskun H, Mendenhall W, Rinaldo A. Prognosis of subglottic carcinoma: is it really worse?. Head Neck. 2019;41:511-521. doi:https://doi.org/10.1002/hed.25172
- Chiari F, Guarino P, Di Martino G. Features related to temporary tracheotomy in patients undergoing Transoral Robotic Surgery (TORS) for supraglottic squamous cell cancer of the larynx: a systematic review. Am J Otolaryngol. 2024;45. doi:https://doi.org/10.1016/j.amjoto.2024.104436
- Russo E, Costantino A, Veneroni M. Transoral laser microsurgery in recurrent laryngeal cancer: a systematic review and meta-analysis. Laryngoscope. 2023;133:1425-1433. doi:https://doi.org/10.1002/lary.30332
- Caporale C, Chiari F, D’Alessio P. Transoral robotic surgery for supraglottic cancer. A review of oncological and functional outcomes compared to open surgery. Acta Otorhinolaryngol Ital. 2024;44:S20-S27. doi:https://doi.org/10.14639/0392-100X-suppl.1-44-2024-N2919
- Chiari F, Cordeschi S, Ingelido C. Transoral robotic surgery for supraglottic laryngeal cancer: a systematic review of functional outcomes and operative features. J Robot Surg. 2025;19. doi:https://doi.org/10.1007/s11701-025-02958-2
- Molteni G, Bassani S, Arsie A. Role of TORS as de-escalation strategy in HPV-related oropharyngeal cancer, what we need to know. Healthcare (Basel). 2024;12. doi:https://doi.org/10.3390/healthcare12101014
- Warner L, O’Hara J, Lin D. Transoral robotic surgery and neck dissection alone for head and neck squamous cell carcinoma: influence of resection margins on oncological outcomes. Oral Oncol. 2022;130. doi:https://doi.org/10.1016/j.oraloncology.2022.105909
- Rodrigo J, Grilli G, Shah J. Selective neck dissection in surgically treated head and neck squamous cell carcinoma patients with a clinically positive neck: systematic review. Eur J Surg Oncol. 2018;44:395-403. doi:https://doi.org/10.1016/j.ejso.2018.01.003
- Machiels J, Leemans R, Golusinski W. ESMO Guidelines Committee. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31:1462-1475. doi:https://doi.org/10.1016/j.annonc.2020.07.011
- Ferlito A, Rinaldo A, Silver C. Elective and therapeutic selective neck dissection. Oral Oncol. 2006;42:14-25. doi:https://doi.org/10.1016/j.oraloncology.2005.03.009
- Deganello A, Ruaro A, Gualtieri T. Central compartment neck dissection in laryngeal and hypopharyngeal squamous cell carcinoma: clinical considerations. Cancers. 2023;15. doi:https://doi.org/10.3390/cancers15030804
- Lucioni M, D’Ascanio L, De Nardi E. Management of paratracheal lymph nodes in laryngeal cancer with subglottic involvement. Head Neck. 2018;40:24-33. doi:https://doi.org/10.1002/hed.24905
- Chabrillac E, Jackson R, Mattei P. Paratracheal lymph node dissection during total (pharyngo-)laryngectomy: a systematic review and meta-analysis. Oral Oncol. 2022;132. doi:https://doi.org/10.1016/j.oraloncology.2022.106017
- Timon C, Toner M, Conlon B. Paratracheal lymph node involvement in advanced cancer of the larynx, hypopharynx, and cervical esophagus. Laryngoscope. 2003;113:1595-1599. doi:https://doi.org/10.1097/00005537-200309000-00035
- Amin M, Edge S, Greene F. AJCC Cancer Staging Manual. Springer; 2017. doi:https://doi.org/10.1007/978-3-319-40618-3
- Wang Z, Zeng Q, Li Y. Extranodal extension as an independent prognostic factor in laryngeal squamous cell carcinoma patients. J Cancer. 2020;11:7196-7201. doi:https://doi.org/10.7150/jca.47700
- Patel A, Vedula S, Shaari A. Extranodal extension in laryngeal squamous cell carcinoma. Laryngoscope Investig Otolaryngol. 2024;9. doi:https://doi.org/10.1002/lio2.1232
- Iocca O, Copelli C, Campo F. Lymph node ratio (LNR) and lymph node yield (LNY) in head and neck cancer: a systematic review and meta-analysis. J Craniomaxillofac Surg. 2025;53:290-300. doi:https://doi.org/10.1016/j.jcms.2024.11.016
- Villaret A, Piazza C, Peretti G. Multicentric prospective study on the prevalence of sublevel IIb metastases in head and neck cancer. Arch Otolaryngol Head Neck Surg. 2007;133:897-903. doi:https://doi.org/10.1001/archotol.133.9.897
- Cappiello J, Piazza C, Giudice M. Shoulder disability after different selective neck dissections (levels II-IV versus levels II-V): a comparative study. Laryngoscope. 2005;115:259-263. doi:https://doi.org/10.1097/01.mlg.0000154729.31281.da
- de Jong A, Manni J. Phrenic nerve paralysis following neck dissection. Eur Arch Otorhinolaryngol. 1991;248:132-134. doi:https://doi.org/10.1007/BF00178921
- Guarino P, Tesauro P, Giordano L. Surgical and radiological perspectives for the spinal accessory nerve passing through a fenestrated internal jugular vein: case series and literature review. J Surg Case Rep. 2024;2024. doi:https://doi.org/10.1093/jscr/rjae099
- Leemans C, Tiwari R, Nauta J. Regional lymph node involvement and its significance in the development of distant metastases in head and neck carcinoma. Cancer. 1993;71:452-6. doi:https://doi.org/10.1002/1097-0142(19930115)71:2<452::aid-cncr2820710228>3.0.co;2-b
- Mimica X, Hanson M, Patel S. Salvage surgery for recurrent larynx cancer. Head Neck. 2019;41:3906-3915. doi:https://doi.org/10.1002/hed.25925
- Malone J, Robbins K. Neck dissection after chemoradiation for carcinoma of the upper aerodigestive tract: indications and complications. Curr Opin Otolaryngol Head Neck Surg. 2010;18:89-94. doi:https://doi.org/10.1097/MOO.0b013e32833693e7
- Thornton A, Laramore G. Technical advances in radiotherapy of head and neck tumors. Hematol Oncol Clin North Am. 1999;13:811-823. doi:https://doi.org/10.1016/s0889-8588(05)70094-0
- Burtness B, Harrington K, Greil R. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet. 2019;394:1915-1928. doi:https://doi.org/10.1016/S0140-6736(19)32591-7
- Mat Lazim N, Abdullah K, Karakullukcu B. Feasibility of salvage selective neck dissection after primary irradiation of pharyngeal and laryngeal carcinoma. ORL J Otorhinolaryngol Relat Spec. 2018;80:10-18. doi:https://doi.org/10.1159/000486371
- van der Putten L, van den Broek G, de Bree R. Effectiveness of salvage selective and modified radical neck dissection for regional pathologic lymphadenopathy after chemoradiation. Head Neck. 2009;3:593-603. doi:https://doi.org/10.1002/hed.20987
- López L, García-Cabo P, Llorente J. Results of salvage neck dissection after chemoradiation in locally advanced head and neck squamous cell carcinoma. Eur Arch Otorhinolaryngol. 2024;281:945-951. doi:https://doi.org/10.1007/s00405-023-08315-z
- Robbins K, Doweck I, Samant S. Effectiveness of superselective and selective neck dissection for advanced nodal metastases after chemoradiation. Arch Otolaryngol Head Neck Surg. 2005;131:965-969. doi:https://doi.org/10.1001/archotol.131.11.965
- Robbins K, Shannon K, Vieira F. Superselective neck dissection after chemoradiation: feasibility based on clinical and pathologic comparisons. Arch Otolaryngol Head Neck Surg. 2007;133:486-489. doi:https://doi.org/10.1001/archotol.133.5.486
- Robbins K, Dhiwakar M, Vieira F. Efficacy of super-selective neck dissection following chemoradiation for advanced head and neck cancer. Oral Oncol. 2012;48:1185-1189. doi:https://doi.org/10.1016/j.oraloncology.2012.05.025
- Lin C, Puram S, Bulbul M. Elective neck dissection for salvage laryngectomy: a systematic review and meta-analysis. Oral Oncol. 2019;96:97-104. doi:https://doi.org/10.1016/j.oraloncology.2019.07.008
- Weiss M, Harrison L, Isaacs R. Use of decision analysis in planning a management strategy for the stage N0 neck. Arch Otolaryngol Head Neck Surg. 1994;120:699-702. doi:https://doi.org/10.1001/archotol.1994.01880310005001
- Hilly O, Gil Z, Goldhaber D. Elective neck dissection during salvage total laryngectomy – A beneficial prognostic effect in locally advanced recurrent tumours. Clin Otolaryngol. 2015;40:9-15. doi:https://doi.org/10.1111/coa.12309
- De Luca P, Di Stadio A, Petruzzi G. A multicenter protocol to assess the prognostic significance of the tumor microenvironment in patients with squamous cell carcinoma of the larynx. Head Neck. 2024;46:2123-2131. doi:https://doi.org/10.1002/hed.27860
- Flach S, Howarth K, Hackinger S. Liquid BIOpsy for MiNimal RESidual DiSease Detection in Head and Neck Squamous Cell Carcinoma (LIONESS) – A personalised circulating tumour DNA analysis in head and neck squamous cell carcinoma. Br J Cancer. 2022;126:1186-1195. doi:https://doi.org/10.1038/s41416-022-01716-7
- Aulakh S, Rosin M, Zhang L. The promise of circulating tumor DNA in head and neck cancer. Cancers (Basel). 2022;14. doi:https://doi.org/10.3390/cancers14122968
- Wang Z, Zeng Q, Li Y. Comparing three-dimensional and two-dimensional deep-learning, radiomics, and fusion models for predicting occult lymph node metastasis in laryngeal squamous cell carcinoma based on CT imaging: a multicentre, retrospective, diagnostic study. EClinicalMedicine. 2024;69. doi:https://doi.org/10.1016/j.eclinm.2024.102343
- Petruzzi G, Coden E, Iocca O. Machine learning in laryngeal cancer: a pilot study to predict oncological outcomes and the role of adverse features. Head Neck. 2023;45:2068-2078. doi:https://doi.org/10.1002/hed.27434
- Filippini D, Carosi F, Querzoli G. Challenges in pathological diagnosis of rare head and neck cancers: national survey and retrospective study. Eur Arch Otorhinolaryngol. 2025;282:6465-6475. doi:https://doi.org/10.1007/s00405-025-09707-z
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 486 times
- PDF downloaded - 116 times