Annual congress report
Vol. 46: 112 TH CONGRESS SIOECHCF - OFFICIAL REPORT 2026
Crico-tracheal resection and anastomosis for primary and secondary tumours of the laryngo-tracheal junction: a single centre series of 78 patients
Summary
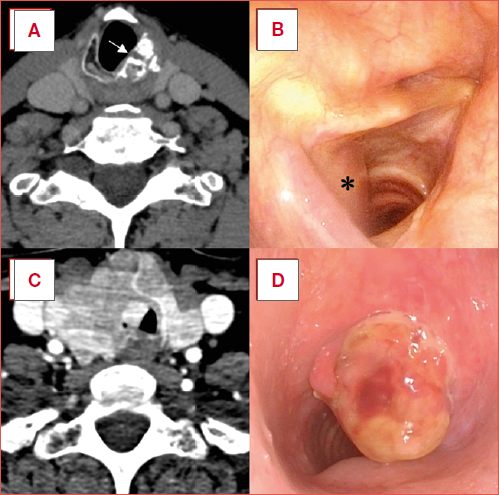
Cover Image
Objective. The aim of this study is to analyse data related to (crico-)tracheal resection and anastomosis [(C)TRA] for primary or secondary tumours involving the laryngo-tracheal junction, focusing on clinical indications, oncological, and functional outcomes.
Methods. A retrospective analysis was conducted on patients treated by (C)TRA from September 1996 to October 2025 in a single academic tertiary referral centre. Patients were distinguished into 5 subgroups based on tumour histology as: 1) advanced thyroid carcinomas involving the airway, 2) cricoid and tracheal chondrosarcomas, 3) minor salivary gland tumours, 4) squamous cell carcinomas, and 5) other rarer histotypes. Primary endpoints included overall (OS), disease-specific (DSS), and laryngectomy-free survivals (LFS).
Results. The cohort consists of 78 patients submitted to 80 (C)TRA distributed among Types A, B, C, and E. The most frequent histotypes were advanced thyroid carcinomas and chondrosarcomas. The final decannulation rate was 97.4% with an overall complication rate of 27.5%. Five-year OS, DSS, and LFS were 65.4, 76.7, and 95%, respectively.
Conclusions. (C)TRA represents an effective surgical strategy for tumours involving the laryngo-tracheal junction, preserving laryngeal functions without compromising oncologic prognosis. Outcomes are excellent for well-differentiated thyroid or cartilaginous tumours, while caution is warranted in highgrade histologies, extrinsic infiltration from metastatic lymph nodes, or previously irradiated patients.
Introduction
Tumours of the laryngo-tracheal junction (i.e. involving the subglottic and/or cervical trachea) are rare and pose significant challenges as their management should ideally simultaneously achieve both oncologic loco-regional control and organ preservation with conservation of airway patency and all laryngo-pharyngo-oesophageal functions. Laryngo-tracheal involvement by neoplastic disease can occur by both intrinsic and extrinsic routes (Cover figure). In particular, intrinsic tumours include primary lesions arising within the proper mucosal, submucosal, or cartilaginous framework of the airway. Squamous cell carcinoma, salivary tumours arising from minor salivary glands, chondromas and chondrosarcomas, and any metastatic lesion reaching the airway via hematogenous spread can be listed in this category. Extrinsic invasion, which represents the predominant epidemiologic scenario, results from secondary airway involvement due to contiguous growth of malignancies arising in the thyroid gland, oesophagus, or lymph nodes of the central compartment of the neck. In both intrinsic and extrinsic lesions, intraluminal tumour growth leads to progressive airflow obstruction, which usually becomes clinically evident only when more than 50% of the airway is compromised (i.e. stenosis comparable to a grade II or more according to the Cotton-Mayer classification) 1, leading to delayed diagnosis of a clinical situation frequently misinterpreted as asthma or other chronic obstructive pulmonary diseases 2,3.
When feasible, surgery still represents the mainstay of treatment for these tumours. Among the available surgical strategies, conservative transoral approaches provide an optimal first-line option aimed at histological sampling and temporary symptomatic relief in case of high-grade stenosis before accurate preoperative staging or airway stenting with palliative intent 4. On the other hand, more aggressive solutions, such as total laryngectomy (TL) extended to the trachea and/or hypopharynx and cervical oesophagus, still represent a valid option in very advanced disease or in patients who are not suitable for conservative surgical strategies due to age, comorbidities or previous treatments 5. Between these 2 extremes, if applied within adequate indications, (crico-)tracheal resection and anastomosis [(C)TRA] can represent an oncologically solid and functionally safe surgical strategy 6-12. In view of the feasibility of airway resection and reconstruction, patient comorbidities and tumour features must be however critically considered in the preoperative setting 13.
The aim of the present article is to analyse data related to (C)TRA for neoplastic diseases treated at a single tertiary, academic, referral centre discussing feasibility, related indications, and results. Procedures will be categorised according to the classification proposed by our Institution in 2014 14 and subsequently refined in other publications 12,15 (Fig. 1), prospectively applied since September 1996, and stratified by histology, highlighting procedure-related complications and oncological outcomes.
Materials and methods
A retrospective analysis was conducted on patients treated by (C)TRA for neoplastic disease between September 1996 and October 2025 at the Unit of Otorhinolaryngology - Head and Neck Surgery of ASST Spedali Civili, University of Brescia, School of Medicine, Brescia, Italy. All patients were deemed eligible for the procedure after evaluation of personal medical history and disease staging. Laryngeal function and endoluminal disease extension were assessed via trans-nasal flexible fibreoptic laryngo-tracheoscopy and/or rigid bronchoscopy in case of pending airway problems, while radiological assessment (by computed tomography [CT] and/or magnetic resonance [MR]) was always carried out to confirm cartilage invasion, lymph node status, and involvement/relationships with surrounding structures such as the hypopharynx, oesophagus, prevertebral fascia, thoracic inlet, major neck and mediastinal vessels.
A prospective dedicated database was created and maintained by the senior author (CP) collecting data regarding surgical procedure, complications, tumour histology, oncological outcomes, and patient survival since 1996. (C)TRA were classified according to the type of resection performed into A1, A2, B, C, and E 12,14,15, length of airway resected, and need for elective postoperative tracheotomy. Complications were classified as immediate (upon awakening in the operating room or intensive care unit [ICU]), early (within 7-10 days), or late (beyond 10 days after surgery), along with the need for related interventions. The decannulation rate for both planned and emergency tracheotomies was assessed. The status of surgical margins on final histopathologic examination (R0 or negative, R1 or positive for microscopic remnants, and R2 or positive for macroscopic remnants) and the requirement for adjuvant therapy were also analysed.
Overall (OS) and disease-specific survivals (DSS) were analysed using the Kaplan-Meier method. OS was defined as the interval between the surgical procedure and death from any cause and patients who were alive at the last follow-up or lost to follow-up were treated as censored observations at the latest available date. DSS was defined as the interval between surgical procedure and death directly attributed to the underlying disease, while patients who remained alive at last documented follow-up or who died from unrelated causes were censored. A further endpoint was laryngectomy-free survival (LFS), defined as the time during which the patient is alive without having undergone TL. Confidence intervals (CI) were calculated at the 95% level using Greenwood’s formula and log transformation was applied to ensure that the confidence limits remained within the 0-1 range.
For the sake of categorisation, to make the analysis more consistent and simplify the discussion, patients were distinguished into 5 subgroups according to tumour histology: 1) thyroid carcinomas with extrinsic infiltration of the airway; 2) chondrosarcomas; 3) tumours originating from minor salivary glands; 4) squamous cell carcinomas of the subglottis and/or trachea; 5) miscellanea of heterogeneous lesions including external airway infiltration from central compartment metastatic lymph nodes or rare histotypes not included in the previous categories.
Results
Overall, the cohort consisted of 78 patients (44 males and 34 females). A total of 80 (C)TRAs were carried out, with 2 males undergoing a second CTRA for disease recurrence. This number represents 38% of the entire series of (C)TRA performed between 1996 and 2025 in our Institution for airway stenoses (n = 209). Mean age was 59 years (range, 19-86). Final histopathological examination identified 34 thyroid cancers (42.6%), 21 chondrosarcomas (26.2%), 8 minor salivary gland tumours (10%), 4 primary squamous cell carcinomas (5%), and 13 other lesions (16.2%).
Regarding the surgical procedure performed, 24 patients (31.2% each) underwent Type A (5 Type A1 and 19 Type A2), B, and C (C)TRA, while 8 patients (10.4%) underwent Type E CTRA. No Type D resection was performed for oncologic reasons. The mean length of resection was 2.4 cm (range, 0.5-3.5). Patients were directly awakened in the operating room at the end of surgery in 68 of 80 procedures, corresponding to an immediate extubation rate of 85%. Among the 19 patients who underwent planned or emergency postoperative tracheostomy, decannulation was successfully achieved in 17 patients (89.5%), corresponding to an overall decannulation rate for the entire series of 97.4%. Overall, 22 surgical complications were recorded across 80 procedures, corresponding to a complication rate of 27.5%.
Median follow-up was 6.6 years. Data regarding OS and DSS are presented in Table I. Overall, estimated one-year OS was 93.5% (95% CI: 88.2-99.2%), 86.6% at 2 years (95% CI: 79.2-94.7%), and 65.4% at 5 years (95% CI: 54.7-78.2%). One-year DSS was 97.3% (95% CI: 93.8-100%), 87.3% at 2 years (95% CI: 79.9-95.4%), and 75.4% at 5 years (95% CI: 65.5-86.8%). Estimated LFS at one and 2 years were 97.3% (95% CI: 93.8-100%), while at 5 years it was 95% (95% CI: 89.5-100%).
Thyroid carcinomas
This subgroup included 34 patients (18 males and 16 females) with thyroid tumours infiltrating the airway. Mean age was 64 years (range, 22-85). Papillary thyroid carcinoma was the predominant histological subtype (n = 24, 70.6%), followed by follicular and mixed papillary-follicular (n = 3 each, 8.8%). De-differentiated or anaplastic tumours were identified in 4 patients (11.8%).
Sixteen patients (47.1%) underwent Type B, 13 (38.2%) Type A (2 Type A1 and 11 Type A2), 4 (11.8%) Type C, and one (2.9%) Type E CTRA. The mean extent of surgical resection was 2.8 cm (range, 2-3.5). A planned temporary tracheostomy was performed in 2 patients (5.9%): one following Type E CTRA, and the other after a Type A2 involving 7 tracheal rings. Negative surgical margins (R0) were achieved in 91.2% of patients. A focally positive margin (R1) was reported in the remaining 3 (8.8%), 2 of which were subsequently found to harbour anaplastic carcinoma on histological evaluation. All except 6 patients (17.6%) were safely extubated in the operating room at the end of the surgical procedure, with fibreoptic evaluation revealing iatrogenic recurrent laryngeal nerve palsy in 2 patients (5.9%). Emergency temporary tracheostomy was required in 8 (23.5%) cases: 6 (17.6%) for surgical and 2 (5.9%) for medical complications, namely respiratory failure caused by pulmonary embolism and abundant broncho-pulmonary secretions. Surgical complications requiring temporary tracheotomy included: glottic oedema in 3 cases (8.8%), anastomotic dehiscence in 2 (5.9%), and postoperative bleeding in one (2.9%). One of the patients experiencing anastomotic dehiscence due to previous radiotherapy (RT) had a second dehiscence managed with laryngo-tracheoplasty with auricular cartilage, deltopectoral flap, and T-tube placement. In this patient tracheostomy was maintained permanently (2.9%). Another patient underwent surgical evacuation of a cervical seroma 15 days after CTRA, without the need for tracheostomy. All the remaining patients with emergent or planned tracheostomy were safely decannulated with an overall decannulation rate of 97.1%. No gastrostomy was ever performed and all patients resumed a normal oral diet before hospital discharge.
Adjuvant therapy was administered in 21 (61.8%) patients: 19 (55.9%) received radioactive iodine (RAI) therapy, one (2.9%) RT, and one (2.9%) a combination of RAI and RT. Four (11.8%) patients had an indication for adjuvant RAI but could not undergo treatment because they already received the maximum cumulative dose before (C)TRA. Information on adjuvant treatment was unavailable for 5 patients. During follow-up, 14 (41.2%) patients experienced distant recurrences (one patient simultaneously locoregional and distant recurrence), while 3 (8.8%) a locoregional recurrence. The median OS was 109.7 months (approximately 9.1 years). Estimated OS at one, 2, and 5 years were 93.7% (95% CI: 85.7-100%), 90.4% (95% CI: 80.6-100%), and 75.6% (95% CI: 61.3-93.2%), respectively. DSS at one, 2, and 5 years were 93.7% (95% CI: 85.3-100%), 90.4% (95% CI: 80.6-100%), and 79.2% (95% CI: 65.5-95.7%), respectively.
Chondrosarcomas
The chondrosarcoma subgroup consisted of 19 patients (13 males and 6 females) submitted to 21 (C)TRA at a mean age of 62 years (range, 40-86). Most cases were low-grade (G1) chondrosarcomas (n = 15, 78.9%), while the remaining (21.1%) were classified as intermediate-grade (G2). Regarding the procedure, 14 patients (73.7%) underwent Type C CTRA, 4 (21%) received a Type E resection, and one (5.3%) a Type A1. Mean length of surgical resection was 2.1 cm (range, 1-3). In most cases (n = 9, 47.4%) the final histopathological report did not specify the status of the resection margins. In 5 cases (26.3%), the margins were reported as free of disease, whereas in 5 (26.3%) residual tumour was documented at least at one resection margin. In 8 patients (42.1%) a planned temporary tracheotomy was performed during surgery. Among the 11 patients who did not receive simultaneous tracheotomy, 9 were directly extubated after surgery, while 2 maintained the orotracheal intubation for 8 and 36 hours, respectively. After extubation in the operating room, one patient required an emergency tracheotomy due to sudden respiratory distress associated with endoscopic evidence of laryngeal oedema and arytenoid anterior dislocation. The most frequently observed complications were laryngeal oedema, reported in 4 patients (21.1%), all of whom already had a tracheotomy in place, and subcutaneous emphysema in 2 (10.5%) cases. Both scenarios resolved spontaneously without further procedures. Two patients (10.5%) required reoperation within 10 days due to postoperative complications: one for bleeding and the other for anastomotic dehiscence on postoperative day 6. Additionally, 2 patients (10.5%) developed anastomotic granulomas after discharge, which were subsequently removed during an office-based procedure or under general anaesthesia by transoral laser microsurgery with CO2 laser. All patients were safely decannulated, with the exception of one patient who underwent Type E CTRA that could not remove the tracheotomy due to chronic obstructive pulmonary disease requiring use of C-PAP overnight (during the day the tracheostomy was always plugged without dyspnoea). None of the patients received adjuvant therapy.
A local recurrence/persistence was documented in 10 cases (52.6%): 2 patients were still managed with conservative surgical treatment (one redo Type C CTRA after a former Type C 77 months before, and one redo Type E after a former Type C 104 months before). These 2 patients showed further tumour relapse during follow-up: the first underwent TL (42 months after the second CTRA, 11 years after the first diagnosis of G1 chondrosarcoma), while the second is currently alive with persistent, slow-growing, asymptomatic G1 disease, under radiological follow-up for nearly 11 years after the first diagnosis. The same applies to the remaining 5 patients with persistent/recurrent disease that is clinically and radiologically stable after 15.7-241 months (mean, 129.4). Among these patients, 5 are alive with disease, and one died due to unrelated comorbidities after 106 months while maintaining stable disease. On the other hand, 2 additional patients underwent TL due to disease progression (at 69 and 6 months after CTRA); the latter died of loco-regional disease 23 months after the initial diagnosis of a very large (> 4 cm) G2 mixoid chondrosarcoma of the cricoid plate. The estimated OS and DSS rates at one and 2 years were 100% and 93.8% (95% CI: 82.6-100%), respectively. The 5-year OS rate was 87.5% (95% CI: 72.7-100%), while the 5-year DSS was 93.8% (95% CI: 82.6-100%). Decannulation rate was 95.3% after CTRA, while organ preservation rate was 85.7%. LFS at one and 2 years were 94.4% (95% CI: 84.4-100%), while at 5 years it was 78.4% (95% CI: 58.6-100%).
Minor salivary gland tumours
Eight patients (10%) were included in this category, consisting of 6 females and 2 males with a mean age of 41 years (range, 19-66). Histologically, the cohort included 5 (62.5%) adenoid cystic carcinomas (ACC), 2 low-grade mucoepidermoid carcinomas (25%), and one pleomorphic adenoma (12.5%). Surgical procedures were evenly distributed across resection types, with 2 patients each (25%) undergoing Type A (one Type A1 and Type A2 each), B, C, and E CTRA. The mean extent of resection was 2.1 cm (range, 1.5-3). In all cases, negative surgical margins were achieved, with no residual disease identified on final pathology. One patient was extubated 24 hours after surgery in the ICU, while all the remaining were successfully extubated on the surgical table. Both patients who underwent Type E CTRA required a planned temporary tracheostomy at the time of surgery, with safe decannulation before discharge (range, 7-10 days after surgery). No patient required an emergency tracheostomy. Postoperative complications were observed in 2 cases: one (12.5%) developed bilateral pneumothorax due to mediastinal pleural laceration requiring chest drains placement for 4 days. One (12.5%) experienced an unintended unilateral vocal cord paralysis that was managed with speech therapy. No other early or late reoperations for complications were recorded in the subgroup. Adjuvant RT was not indicated for 5 patients (62.5%). Two (25%) had undergone RT prior to surgery, and one (12.5%) underwent it as adjuvant treatment. No local or regional recurrences were observed during follow-up. One patient (12.5%) developed distant bone metastases and subsequently died of disease 18 months after CTRA and adjuvant RT. All the remaining patients were alive and with no evidence of disease at last follow-up. Estimated one-year OS and DSS were 100%, while 2- and 5-year OS and DSS rates were 87.5% (95% CI: 67.3-100%). Decannulation and organ preservation rates were 100%.
Squamous cell carcinomas
This subgroup included 4 patients (2 males and 2 females) with a mean age of 59 years (range, 48-66), all treated for subglottic or tracheal SCC. In 3 patients (75%), the tumour was a recurrence of previously treated glottic SCC managed with transoral laser microsurgery, whereas in one case (25%) the procedure was performed as a primary treatment. Regarding the type of resection, 3 (75%) underwent Type B and one Type C CTRA. The mean length of resection was 2.6 cm (range, 2-3 cm). Clear surgical margins were achieved in 3 patients (75%), while one case (25%) showed focal carcinoma in situ at the histopathological final report. All patients were directly extubated after surgery, and no patient required postoperative tracheotomy. Considering surgical complications, one patient (25%) underwent flexible bronchoscopy on the 10th postoperative day for obstructive fibrin removal. Postoperative adjuvant RT was administered to 2 patients (50%), one did not receive adjuvant RT due to prior irradiation, and one had no indication for adjuvant RT. During follow-up, one patient developed a locoregional recurrence and died of disease progression after 7.4 years. Another patient developed a regional recurrence, which was managed with combined CRT, and remains free of disease at last follow-up (August 2025). Estimated OS and DSS rates at one, 2 and 5 years were 100%. Decannulation and organ preservation rates were 100%.
Other tumours
A total of 13 patients were included in this subgroup (9 males and 4 females) with a mean age of 55 years (range, 24-70). Final histopathological reports demonstrated 6 cases (46.1%) of level VI lymph node metastases of previous disease (3 from oral cavity, 2 from laryngeal, and one from oropharyngeal cancers), 4 (30.8%) metastases to the thyroid gland with airway invasion (2 from rectal adenocarcinoma, one from clear cell renal carcinoma, and one from leiomyosarcoma), one (7.7%) tracheal spindle cells tumour, one (7.7%) tracheal giant cell tumour, and one (7.7%) subglottic schwannoma. Regarding surgical management, 8 patients (61.5%) underwent Type A CTRA (1 Type A1 and 7 Type A2), 3 (23.1%) Type B, and 2 (15.4%) Type C, with a mean resection length of 2.3 cm (range, 0.5-3.5). All patients achieved R0 resection according to the final histopathological report, except for one case with an R1 margin (involved by clear cell renal carcinoma). No patient required elective or emergency tracheotomy, one patient was extubated after 12 hours of ICU stay, while all the remaining were directly extubated after surgery. No early complications were encountered. One patient (who previously underwent CRT for metastatic lymph nodes from laryngeal cancer invading the trachea and oesophagus) developed a posterior anastomotic dehiscence with tracheoesophageal fistula on the 19th postoperative day, requiring subsequent TL with radial forearm free flap reconstruction. Regarding adjuvant treatment, RT would have been indicated in 5 cases (38.5%), but was not administered because the patients had previously undergone irradiation. In 7 patients (53.8%) no adjuvant therapy was indicated. Adjuvant (C)RT was performed in one patient (7.7%). During follow-up, one patient (7.7%) developed a regional recurrence that was managed surgically, and remained disease-free at last follow-up. Two patients (15.4%) experienced a local recurrence that was not amenable to further surgery, and 6 (46.1%) developed distant metastases involving lungs, bone, or brain. Analysing the patients with extrinsic airway infiltration for Level VI nodal metastases, the estimated OS and DSS were 100% at one year, 80% (95% CI: 51.6-100%) at 2 years, and 20% (95% CI: 3.5-100%) at 5 years. The decannulation rate after CTRA was 100%, while the organ preservation rate was 92.3%.
Discussion
The present study reports the outcomes of one of the largest available head and neck cohort of patients surgically treated by (C)TRA for primary and secondary neoplastic diseases. This analysis includes a broad spectrum of histological subtypes, which were evaluated separately to allow a more comprehensive assessment of the role of this conservative approach across different oncological scenarios. The results consistently demonstrate a high rate of surgical success with low complication rates overall, excellent chances of definitive decannulation (97.4%), and satisfactory oncological disease control. These findings support (C)TRA as an oncologically adequate surgical option in patients with neoplastic involvement of the airway. However, given the technical complexity of the procedure and the potential for life-threatening complications, we cannot overemphasise the importance of proper selection, since the patient profile, length, location, degree of airway involvement, and tumour features are the key determinants of successful outcomes.
Based on our experience, patients must be fit for major surgery in terms of general conditions and comorbidities, and adequately motivated to undergo a complex surgical pathway 13. Caution should be exercised in previously irradiated patients, in whom tissue and laryngeal function impairment may significantly increase the risk of complications and compromise outcomes 14,16. The lesions should involve less than 60% of the cricoid circumference on the axial plane with a cranio-caudal extension of resection of less than 5.5 cm. In this respect, however, one should argue that this maximal extent of airway resection is usually possible only in young patients with an elastic and compliant laryngo-tracheal axis, while Piazza et al. demonstrated a considerable increase in terms of anastomotic dehiscence for resections longer than 4 cm 14. This should be especially taken in mind when dealing with oncologic patients, who are usually in the second half of their life expectancy. At least one functioning cricoarytenoid unit must be always preserved, and there should be no evidence of invasion of the glottic plane, hypopharynx, or oesophageal mucosa. Limited oesophageal siero-muscular layer involvement may be managed by careful shaving resection, even though this is one of the most unfavourable prognosticators in terms of loco-regional recurrence. Thyroid cartilage should be untouched or involved only in its inferior subglottic half or external layer.
Respecting such indications, excellent results were observed in our cohort of selected histological subgroups, namely non-anaplastic thyroid carcinomas, G1-G2 chondrosarcomas, and tumours of the minor salivary glands. Conversely, outcomes were significantly less favourable in patients presenting with extrinsic airway invasion from regional lymph nodes harbouring SCC metastases or distant metastatic involvement of the airway, showing a DSS rate which remains poor despite surgical management. (C)TRA should be avoided in chondrosarcomas exceeding 4 cm in maximum diameter: in such a case, in fact, even if the airway is still manageable conservatively, there is a non-negligible chance to find at definitive evaluation of the entire surgical specimen an undifferentiated-high-grade (G3) component of the chondrosarcoma itself or other more aggressive variants with higher local recurrence and distant metastases rates 17.
Finally, a special consideration should be reserved to patients with a history of prior RT. The feasibility of a conservative approach can only be determined intraoperatively upon assessment of tissue viability. The use of revascularised flaps such as radial forearm or antero-lateral thigh free flaps for anastomotic covering should be always considered. Furthermore, in view of the increased risk of potentially life-threatening complications, in this case clinical safety should prevail over organ-sparing objectives.
When dealing with intrinsic airway tumours managed with radical resection, our survival outcomes are consistent with previously published experiences. Gaissert et al. 18 published a series of 25 patients treated by laryngo-tracheoplastic procedures for primary tumours of the proximal airway, with favourable long term outcomes (5-year OS, 79%). In this context slow growing, oncologically favourable lesions such as G1-G2 chondrosarcomas represent the best indications for CTRA over palliative transoral laser debulking or TL. In well selected patients, in fact, CTRA allows the possibility of a complete resection, offering good quality of life in terms of voice and normal swallow without compromising survival 8-10,12,19-22.
Primary subglottic or tracheal SCC are a rare and biologically aggressive entity, which is usually managed with more radical treatment strategies, most commonly TL, to ensure oncological safety 23. In our series, most cases of SCC consisted of selected small recurrences of previously treated glottic carcinomas, with a 5-year DSS of 100% after (C)TRA. This percentage must be interpreted with caution, however, since it represents the outcomes of a highly selected population. Other authors providing data on primary SCC of the trachea and carina report lower OS as expected for wider, heterogeneous series 24.
Overall, primary salivary tumours arising from the subglottis or trachea remain a rare finding, for which surgery still represents the treatment of choice in most reported series 11,12,25-27. Evidence specifically aimed to address laryngeal-preserving approaches in view of long-term outcomes and complications remains limited. However, perineural spread and extensive submucosal growth of these tumours usually make (C)TRA and other function-sparing approaches at risk of R1 margins, being extended TL the most frequently needed kind of surgical resection. A recent systematic review by Ran et al. 28, focusing on tracheal ACC, reported a 5-year OS after surgery alone of 86.4%, in line with our findings.
Regarding extrinsic airway infiltration, thyroid gland cancer represents by far the main indication for (C)TRA in every busy head and neck cancer department 6,7,29,30. This approach is particularly justified in well-differentiated tumours, where long-term survival can be effectively achieved despite the locally advanced stage of disease, with a 5-year OS of 87.3% in our series for well-differentiated cancers, with only a 3% rate of tracheotomy dependence. These data are consistent with the literature, which confirms, by contrast, the low survival rates for poorly differentiated or anaplastic tumours 6,31-35. However, literature findings should be interpreted with caution, as studies often include heterogeneous thyroid histotypes managed through diverse surgical approaches. In this regard, a recent case series by Staubitz-Vernazza et al. 36 reported a 2-year OS of 82%, with survival being generally higher in patients undergoing CTRA compared with other surgical techniques (i.e. window resection or other non-circumferential airway resection procedures carrying a higher risk of R1 margins).
This study is not without limitations. Firstly, the retrospective design (even though on a prospectively collected database managed by the same senior author over a period of 30 years) and the heterogeneity of the population inherently expose the analysis to selection bias, which could limit the applicability of our results to other settings. In addition, this series includes a highly heterogeneous cohort collected over an extended time, during which relevant advances in diagnostic workup and therapeutic strategies have occurred. To mitigate the impact of pathological heterogeneity, a histology-based categorisation was applied. Finally, the study population consists of particularly complex patients, many of whom presented with locally-advanced disease or metastatic pattern at diagnosis, factors that may have negatively affected survival outcomes.
Conclusions
(C)TRA represents a balanced and effective surgical strategy for managing both primary and secondary tumours affecting the laryngo-tracheal junction, being a reliable alternative to more radical procedures like TL, and thus preserving essential laryngeal functions without compromising long-term prognosis. Our findings on a large monocentric case series demonstrate that, when strict selection criteria are applied, high rates of decannulation and satisfactory oncological control can be achieved. While the procedure offers excellent functional and survival outcomes, for well-differentiated thyroid carcinomas, most G1-G2 chondrosarcomas and salivary tumours, caution is warranted in cases of high-grade or undifferentiated histologies, extrinsic airway infiltration by Level VI lymph nodes metastases, and previously irradiated patients. Future collaborative studies will allow for the improvement of patient stratification and the refinement of surgical indications, further optimising long-term functional and oncological results.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
DL, CM, CP: data acquisition, study conception and design, critical revision of the article and final approval of the version to be published; DL, CM: data analysis, article drafting; FDB, GZ, GB, CM, GT: critical revision of the article and final approval of the version to be published.
Ethical consideration
This study was approved by the Institutional Ethics Committee of the University of Brescia (protocol number: 4268). The research was conducted ethically, with all study procedures being performed in accordance with the requirements of the World Medical Association’s Declaration of Helsinki. Written informed consent was obtained from each patient for study participation and data publication.
History
Received: January 21, 2026
Accepted: February 2, 2026
Figures and tables
Figure 1. Diagram representing the University of Brescia classification of (C)TRA.
| Time (y) | NR | NE | OS (%) | NR | NE | DSS (%) | |
|---|---|---|---|---|---|---|---|
| Thyroid carcinoma | 1 | 28 | 2 | 93.7 | 28 | 2 | 93.7 |
| 2 | 26 | 1 | 90.4 | 26 | 1 | 90.4 | |
| 5 | 17 | 4 | 75.6 | 17 | 3 | 79.2 | |
| Chondrosarcoma | 1 | 18 | 0 | 100 | 18 | 0 | 100 |
| 2 | 15 | 1 | 93.8 | 15 | 1 | 93.8 | |
| 5 | 10 | 1 | 87.5 | 10 | 0 | 93.8 | |
| Minor salivary glands tumours | 1 | 8 | 0 | 100 | 8 | 0 | 100 |
| 2 | 7 | 1 | 87.5 | 7 | 1 | 87.5 | |
| 5 | 4 | 0 | 87.5 | 4 | 0 | 87.5 | |
| Squamous cell carcinoma | 1 | 4 | 0 | 100 | 4 | 0 | 100 |
| 2 | 3 | 0 | 100 | 3 | 0 | 100 | |
| 5 | 3 | 0 | 100 | 3 | 0 | 100 | |
| Level VI node metastasis | 1 | 5 | 0 | 100 | 5 | 0 | 100 |
| 2 | 4 | 0 | 80 | 4 | 0 | 80 | |
| 5 | 0 | 3 | 20 | 0 | 3 | 20 | |
| Total | 1 | 71 | 5 | 93.5 | 71 | 2 | 97.3 |
| 2 | 59 | 5 | 86.6 | 59 | 7 | 87.3 | |
| 5 | 37 | 13 | 65.4 | 37 | 7 | 75.4 | |
| NR: number at risk; NE: number of events. | |||||||
References
- Myer C, O’Connor D, Cotton R. Proposed grading system for subglottic stenosis based on endotracheal tube sizes. Ann Otol Rhinol Laryngol. 1994;103:319-323. doi:https://doi.org/10.1177/000348949410300410
- Wu C, Shepard J. Tracheal and airway neoplasms. Semin Roentgenol. 2013;48:354-364. doi:https://doi.org/10.1053/j.ro.2013.03.018
- Li Y, Peng A, Yang X. Clinical manifestation and management of primary malignant tumors of the cervical trachea. Eur Arch Otorhinolaryngol. 2014;271:225-235. doi:https://doi.org/10.1007/s00405-013-2429-9
- Marchioni A, Moretti A, Tonelli R. Stent and resection anastomosis in patients with complex tracheal stenosis: the Stars retrospective multicenter trial. Interdiscip Cardiovasc Thorac Surg. 2025;40. doi:https://doi.org/10.1093/icvts/ivaf261
- Piazza C, Lancini D, Paderno A. Cervical exenteration and its variants for locally advanced thyroid cancer: when, why, and how?. Curr Opin Otolaryngol Head Neck Surg. 2023;31:65-72. doi:https://doi.org/10.1097/MOO.0000000000000873
- Piazza C, Del Bon F, Barbieri D. Tracheal and crico-tracheal resection and anastomosis for malignancies involving the thyroid gland and the airway. Ann Otol Rhinol Laryngol. 2016;125:97-104. doi:https://doi.org/10.1177/0003489415599000
- Piazza C, Lancini D, Tomasoni M. Tracheal and cricotracheal resection with end-to-end anastomosis for locally advanced thyroid cancer: a systematic review of the literature on 656 patients. Front Endocrinol (Lausanne). 2021;12. doi:https://doi.org/10.3389/fendo.2021.779999
- Piazza C, Del Bon F, Grazioli P. Organ preservation surgery for low- and intermediate-grade laryngeal chondrosarcomas: analysis of 16 cases. Laryngoscope. 2014;124:907-912. doi:https://doi.org/10.1002/lary.24416
- Piazza C, Paderno A, Nicolai P. Conservative surgery for laryngeal chondrosarcoma: a review of the most recently proposed approaches. Curr Opin Otolaryngol Head Neck Surg. 2017;25:93-100. doi:https://doi.org/10.1097/MOO.0000000000000337
- Ruller K, Sittel C, Kolmel J-C. Organ preservation strategies in laryngeal chondrosarcoma. Laryngoscope. 2022;132:838-843. doi:https://doi.org/10.1002/lary.29826
- Montenegro C, Mattavelli D, Lancini D. Treatment and outcomes of minor salivary gland cancers of the larynx and trachea: a systematic review. Acta Otorhinolaryngol Ital. 2023;43:365-374. doi:https://doi.org/10.14639/0392-100X-N2635
- Piazza C, Lancini D, Zigliani G. Hemicricoidectomy with modified rotational thyro-crico-tracheal anastomosis: a newborn in the family of crico-tracheal resection and anastomosis techniques. Acta Otorhinolaryngol Ital. 2024;43:382-389. doi:https://doi.org/10.14639/0392-100X-N2623
- Monnier P, Dikkers F, Eckel H. Preoperative assessment and classification of benign laryngotracheal stenosis: a consensus paper of the European Laryngological Society. Eur Arch Otorhinolaryngol. 2015;272:2885-2896. doi:https://doi.org/10.1007/s00405-015-3635-4
- Piazza C, Del Bon F, Paderno A. Complications after tracheal and cricotracheal resection and anastomosis for inflammatory and neoplastic stenoses. Ann Otol Rhinol Laryngol. 2014;123:798-804. doi:https://doi.org/10.1177/0003489414538764
- Piazza C, Lancini D, Filauro M. Post-COVID-19 airway stenosis treated by tracheal resection and anastomosis: a bicentric experience. Acta Otorhinolaryngol Ital. 2022;42:99-105. doi:https://doi.org/10.14639/0392-100X-N1952
- Fiz I, Filauro M, Sampieri C. Analysis of complications in (crico-)tracheal resection anastomosis in adults: a multicenter study. Laryngoscope. 2023;133:2910-2919. doi:https://doi.org/10.1002/lary.30635
- Piazza C, Montenegro C, Tomasoni M. Aggressive subtypes of laryngeal chondrosarcoma and their clinical behavior: a systematic review. Oncol Ther. 2025;13:49-67. doi:https://doi.org/10.1007/s40487-024-00323-1
- Gaissert H, Grillo H, Shadmehr B. Laryngotracheoplastic resection for primary tumors of the proximal airway. J Thorac Cardiovasc Surg. 2005;129:1006-1009. doi:https://doi.org/10.1016/j.jtcvs.2004.07.043
- Cronkite D, Moffatt C, Tam K. Contemporary surgical approaches in managing laryngeal chondrosarcoma: a scoping review. Laryngoscope. 2025;135:2241-2248. doi:https://doi.org/10.1002/lary.32068
- Lopes P, Nascimento J, Rocha G. Laryngeal chondrosarcoma, a 30-year series. Acta Otorrinolaringol Esp (Engl Ed). 2025;76:20-24. doi:https://doi.org/10.1016/j.otoeng.2024.09.004
- Schleich M, Laccourreye L, Marianowski R. Treatment strategy in laryngeal chondrosarcoma: a multicenter study of 43 cases. Eur Arch Otorhinolaryngol. 2024;281:883-890. doi:https://doi.org/10.1007/s00405-023-08248-7
- Álvarez-Calderón-Iglesias O, Pèrez-Sayans M, Hurtado-Ruzza R. Survival outcomes in laryngeal chondrosarcoma: a systematic review. Acta Otorhinolaryngol Ital. 2022;42:502-515. doi:https://doi.org/10.14639/0392-100X-N1912
- Mann H, Seligman K, Colwell N. Management of subglottic cancer. Otolaryngol Clin North Am. 2023;56:305-312. doi:https://doi.org/10.1016/j.otc.2022.11.001
- Gaissert H, Grillo H, Shadmehr M. Long-term survival after resection of primary adenoid cystic and squamous cell carcinoma of the trachea and carina. Ann Thorac Surg. 2004;78:1889-1896. doi:https://doi.org/10.1016/j.athoracsur.2004.05.064
- Joshi P, Bhattacharya K, Bal Menon M. Malignant minor salivary gland neoplasms of larynx: our experience. Otolaryngol Pol. 2023;77:1-7. doi:https://doi.org/10.5604/01.3001.0053.4040
- Chiari F, Di Martino G, Caporale C. Analysis of local, regional, and distant recurrence of disease in mucoepidermoid tumors of larynx: a systematic review. Head Neck. 2024;46:1822-1834. doi:https://doi.org/10.1002/hed.27767
- Ganly I, Patel S, Coleman M. Malignant minor salivary gland tumors of the larynx. Arch Otolaryngol Head Neck Surg. 2006;132:767-770. doi:https://doi.org/10.1001/archotol.132.7.767
- Ran J, Qu G, Chen X. Clinical features, treatment and outcomes in patients with tracheal adenoid cystic carcinoma: a systematic literature review. Radiat Oncol. 2021;16. doi:https://doi.org/10.1186/s13014-021-01770-0
- Gaissert H, Honings J, Grillo H. Segmental laryngotracheal and tracheal resection for invasive thyroid carcinoma. Ann Thorac Surg. 2007;83:1952-1959. doi:https://doi.org/10.1016/j.athoracsur.2007.01.056
- Abd-Elfattah A, Tawfik A, Hossam A. Thyroidectomy with tracheal/cricotracheal resection anastomosis for different pathologies: optimizing the outcomes. Int Arch Otorhinolaryngol. 2025;29:1-8. doi:https://doi.org/10.1055/s-0045-1810076
- Wada N, Nakayama H, Masudo Y. Clinical outcome of different modes of resection in papillary thyroid carcinomas with laryngotracheal invasion. Langenbecks Arch Surg. 2006;391:545-549. doi:https://doi.org/10.1007/s00423-006-0106-9
- Brauckhoff M. Classification of aerodigestive tract invasion from thyroid cancer. Langenbecks Arch Surg. 2014;399:209-216. doi:https://doi.org/10.1007/s00423-013-1142-x
- Hartl D, Zago S, Leboulleux S. Resection margins and prognosis in locally invasive thyroid cancer. Head Neck. 2014;36:1034-1038. doi:https://doi.org/10.1002/hed.23406
- Kim B-Y, Choi J-E, Lee E. Prognostic factors for recurrence of locally advanced differentiated thyroid cancer. J Surg Oncol. 2017;116:877-883. doi:https://doi.org/10.1002/jso.24740
- Liu Y, Song Y, He Y. Surgical management and outcomes of T4a papillary thyroid carcinoma: a single-centre study of 602 cases. Endocrine. 2025;87:648-657. doi:https://doi.org/10.1007/s12020-024-04026-5
- Staubitz-Vernazza J, Schwind S, Lozan O. A 16-year single-center series of trachea resections for locally advanced thyroid carcinoma. Cancers (Basel). 2023;16. doi:https://doi.org/10.3390/cancers1601016
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 366 times
- PDF downloaded - 128 times