Annual congress report
Vol. 46: 112 TH CONGRESS SIOECHCF - OFFICIAL REPORT 2026
Radiomics in laryngeal squamous cell carcinoma: state of the art
Authors
Sonia Lucchese
 , Francesca Laganaro
, Gerardo Petruzzi
, Antonello Vidiri
, Francesca Laganaro
, Gerardo Petruzzi
, Antonello Vidiri
Summary
Cover Image
Laryngeal squamous cell carcinoma (LSCC) is one of the most common malignancies of the head and neck, and accurate staging is essential for optimal therapeutic decision-making. However, discrepancies between clinical-radiological staging and pathological findings, particularly in the assessment of thyroid cartilage invasion and lymph node involvement, may result in inappropriate treatment decisions. Radiomics has recently emerged as a quantitative imaging approach capable of extracting high-dimensional features from medical images, providing objective biomarkers that reflect tumour heterogeneity beyond visual assessment. This narrative review summarises current evidence on radiomics applications in LSCC, including staging, cartilage invasion assessment, nodal evaluation, and prognostic stratification, and outlines the main steps of the radiomic workflow together with current methodological challenges. Recent studies indicate that radiomics, particularly when integrated with deep learning and clinical data, improves diagnostic and prognostic performance compared with conventional imaging alone. However, methodological heterogeneity and limited external validation still restrict routine clinical implementation, and further standardisation and prospective multicentre validation are required before widespread clinical adoption.
Introduction
Head and neck (HN) cancer represents the 7th most common malignancy worldwide 1. Within this group, laryngeal cancer ranks among the most frequent tumours, with approximately 190,000 new cases and over 100,000 deaths worldwide 2. Squamous cell carcinoma (SCC) constitutes the predominant histological subtype 3.
Tobacco and alcohol consumption are the main established risk factors for laryngeal SCC (LSCC) 4,5. Clinical presentation varies according to tumour location and extent. Glottic carcinomas typically present early with dysphonia, whereas supraglottic tumours tend to manifest at more advanced stages and are often associated with late symptoms such as pain, persistent dysphonia, or dysphagia 6.
Preoperative treatment planning is mainly based on clinical staging derived from endoscopic evaluation, including indirect and flexible laryngoscopy 7. Narrow band imaging further enhances diagnostic accuracy, with reported sensitivity and specificity of 97% and 92.5%, respectively, for detecting LSCC and precursor lesions 8.
Imaging also plays a critical role in staging. Computed tomography (CT) is particularly effective for evaluating potential bone invasion, while positron emission tomography (PET) – CT is useful for detecting recurrence, assessing local disease spread, and identifying distant metastases in advanced stages 9. Surface-coil magnetic resonance imaging (MRI) offers superior diagnostic performance exhibiting higher sensitivity (80%) and specificity (92.9%) compared to CT (60% and 85.7%, respectively) in assessing thyroid cartilage involvement. MRI accuracy is further enhanced among experienced radiologists and shows improved interobserver agreement 10,11.
Despite these diagnostic advances, the accuracy of clinical staging remains limited, as endoscopy and conventional imaging frequently yield stage assessments that do not correspond to the pathological findings. This limitation is clinically relevant, as staging directly influences therapeutic decision-making and the selection of surgical options; discrepancies between clinical-radiological staging and pathological findings may result in inappropriate surgical management, leading either to delayed definitive treatment or to overtreatment. Assessment of thyroid cartilage invasion is particularly challenging. Endoscopy cannot directly evaluate cartilage involvement, and both CT and MRI frequently overestimate invasion, potentially resulting in unnecessary total laryngectomy 12,13.
To overcome the limitations of qualitative, morphology-based imaging, which is subject to both inter- and intra-observer variability, radiomics has emerged as a quantitative imaging approach capable of capturing tumour heterogeneity. Radiomics extracts high-dimensional quantitative features from imaging data, providing biomarkers that reflect underlying properties which are not apparent on visual assessment. Increasing evidence indicates that radiomics can enhance diagnostic accuracy and predictive modelling, supporting more reliable staging, prediction of treatment response, and prognostic stratification in LSCC 14.
Radiomics
The suffix “-omics” denotes various sources of large-scale data and is preceded by the name of the biological or physical domain from which such data are derived. Accordingly, the aim of radiomics is to extract quantitative information from radiological images using advanced computational methods 15. By converting images into high-dimensional data, radiomics enables the characterisation of tumour heterogeneity beyond what is visually appreciable, potentially supporting clinical decision-making within the framework of precision oncology.
Radiomic features can be categorised into intensity-based (first-order), shape-related, and texture-based measurements 16. Among these, texture features have been investigated as surrogate markers of tumour heterogeneity, enabling the extraction of many quantitative characteristics that may reflect underlying biological complexity 17. Numerous studies have evaluated radiomic features extracted from different imaging modalities – such as CT, PET, and MRI – across a wide range of tumour types 18-23, also assessing their reproducibility and variability in diverse clinical settings 18,24-26.
Radiomic features have demonstrated significant predictive and prognostic values, showing correlations with tumour histology, grade, stage 27,28, and survival outcomes 18,19,22-25,27.
Furthermore, radiogenomic studies have identified associations between radiomic characteristics and gene expression profiles 18,21,23,29,30, highlighting the potential role of radiomics in treatment personalisation across different oncological contexts.
However, further methodological development, increased standardisation, and large-scale validation are required to achieve true clinical implementation. As highlighted by Traverso et al. 31, many radiomic features are highly sensitive to variations in image acquisition, reconstruction, preprocessing, and segmentation parameters, underscoring the need for reproducible pipelines and genuinely stable radiomic biomarkers.
These considerations are particularly relevant in HN oncology, and specifically in LSCC, where anatomical complexity, motion artifacts, cartilage involvement, and small tumour volumes pose additional challenges for image-based quantitative analysis. This review therefore aims to summarise the main concepts, current evidence, and ongoing challenges of radiomics, focusing on its application to LSCC.
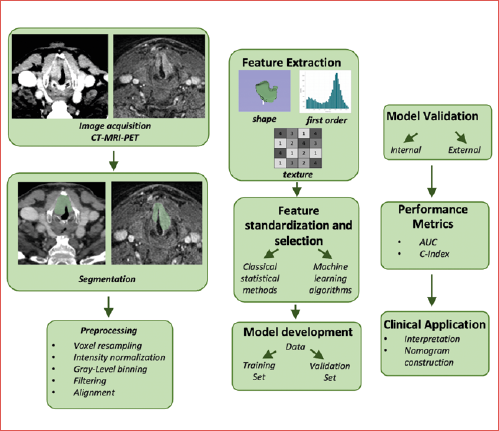
Radiomic workflow
The radiomic workflow requires a multidisciplinary approach and consists of several sequential phases, each of which can substantially influence the reliability of extracted features.
CT is the most used modality in radiomic studies, although the approach can be extended to PET, MRI, and ultrasound (US). CT and PET-CT provide inherently quantitative values, whereas MRI and US require a higher degree of standardisation to account for scanner- and protocol-dependent variability and ensure consistency. Harmonised acquisition protocols are essential to minimise variability 32, and images should be exported in lossless Digital Imaging and COmmunications in Medicine (DICOM) format. In parallel, clinical data must be consistently collected and verified before integration with radiomic features 33.
Preprocessing steps – including intensity normalisation, bias-field correction, noise reduction, discretisation, resam-pling, and filtering (e.g., Laplacian of Gaussian [LoG)] wavelet) – are applied to harmonise image data and improve feature comparability, although they may influence extracted feature values. In MRI-based radiomics, intensity normalisation is generally required to mitigate scanner-related variability 34, bias-field correction reduces intensity inhomogeneities 35, while spatial resampling is required to ensure comparability of voxel-dependent features 36,37.
Segmentation may be manual, semi-automatic, or fully automatic, and can encompass the tumour volume, subregions (“habitats”), or peritumoural areas 38,39. Automatic methods show greater reproducibility 25 but still require radiologist review; manual segmentation, conversely, necessitates estimation of intra- and interobserver variability.
Handcrafted radiomic features can be broadly categorised into several families. Morphological (shape-based) features describe tumour geometry and size, including volume, surface area, sphericity, and compactness. Intensity-based (first-order) features quantify the distribution of voxel intensities within the tumour, such as mean, median, variance, skewness, and entropy. Texture-based features capture spatial relationships between voxel intensities and tumour heterogeneity and are derived from matrices such as the Grey Level Co-occurrence Matrix (GLCM), Grey Level Run Length Matrix (GLRLM), Grey Level Size Zone Matrix (GLSZM), Grey Level Dependence Matrix (GLDM), and Neighborhood Grey Tone Difference Matrix (NGTDM). Finally, higher-order features are obtained from mathematical transforms or filtered images, including wavelet decomposition, LoG, and local binary patterns (LBP). Definitions and calculation methods for all these features are standardised according to the Image Biomarker Standardisation Initiative (IBSI) 37.
Predictive modelling typically integrates radiomic features with clinical data and requires independent validation, or alternatively, rigorous cross-validation. Statistical comparability between training and validation sets must be verified. Feature stability should be assessed using the Intraclass Correlation Coefficient (ICC), with thresholds between 0.75 and 0.90 considered acceptable 40,41, preferably evaluated through test-retest studies.
Dimensionality reduction and feature selection – using filter, wrapper, or embedded methods, or regularisation techniques such as Least Absolute Shrinkage and Selection Operator (LASSO), ridge regression, or elastic net – are essential to prevent redundancy and overfitting.
Software selection should consider transparency, update frequency, Picture Archiving and Communication System (PACS) integration, and adherence to IBSI standards; however, compliance with IBSI alone does not guarantee reproducibility, which also depends on parameter harmonisation and consistency across software versions 42.
Radiomic workflow is summarised in the Cover figure.
Materials and methods
Search strategy
A narrative review of the recent literature was performed on PubMed/MEDLINE and Scopus database by 2 independent reviewers (S.L. and A.V.). The search strategy used combinations of the terms “laryngeal cancer”, “radiomics”, “deep learning (DL)”, “MRI”, “CT”, and “PET-CT.” Original articles, review papers, and imaging studies relevant to the application of radiomics in staging, prognosis, and prediction of treatment response in LSCC were considered eligible. The aim was to identify and select the most representative studies for a critical discussion of the current state of the art.
Eligibility criteria
Original articles applying radiomics and/or DL to LSCC for diagnostic purposes, staging, prognostic assessment, or prediction of treatment response were included. Studies involving mixed HNSCC cohorts were included only when extractable LSCC-specific data were available or when the study was deemed methodologically relevant. Review articles and methodological papers were considered to contextualise the current state of the art. Given the narrative nature of this review, the literature search was not intended to be exhaustive but rather focused on recent, clinically relevant, and methodologically representative studies, with particular emphasis on publications from the last decade. Earlier seminal contributions were selectively included when necessary to provide historical or methodological context. Conference abstracts, case reports, studies not incorporating quantitative imaging feature analysis, and publications without accessible full text were excluded. Only articles published in English were considered eligible.
Population description
Recent scoping and systematic reviews identified 30 radiomics studies specifically focused on LSCC. Among these, most applied contrast-enhanced CT (18 studies), while fewer used multiparametric MRI (2 studies) or 18F-FDG PET-CT (3 studies). Additional studies investigated mixed HNSCC populations or incorporated radiomics with advanced Artificial Intelligence (AI) methodologies such as federated learning or explainable AI.
Results
Recently, several studies have explored the application of radiomics to the staging of laryngeal carcinoma, with particular focus on T classification, assessment of cartilage invasion, and N staging. Table I summarises the performance metrics and major findings of the studies reviewed.
Radiomic workflow
Radiomic studies on laryngeal carcinoma exhibit substantial methodological heterogeneity, although several recurring technical elements reflect present research standards in the field. All study objectives are depicted in Table II.
Most CT-based studies used post-contrast acquisitions, followed by manual three-dimensional segmentation of the tumour volume and standardised preprocessing procedures, including isotropic resampling, intensity discretisation, and – when required – signal normalisation 43-45. Feature extraction typically incorporated morphological, first-order, and texture descriptors, using standardised radiomic definitions largely consistent with IBSI recommendations; in some studies, these features were further supplemented with wavelet-filtered features or habitat-oriented approaches to better characterise intralesional heterogeneity 46,47.
Feature selection predominantly relied on regularisation techniques, most notably LASSO, whereas predictive modelling frequently employed logistic regression or Cox proportional hazards models. More recent studies have explored DL-based approaches and hybrid frameworks integrating handcrafted radiomic features with DL-derived representations to improve predictive performance 48-50.
Only a minority of CT-based studies incorporated independent external validation; for example, Kang et al. 51 relied on internal cohort splitting, highlighting a common methodological limitation and underscoring the need for more robust, multi-institutional, validation strategies.
MRI-based studies, in contrast, implemented more complex analytical pipelines, reflecting the non-quantitative nature and higher intrinsic variability of MRI signal intensities. These investigations predominantly adopted multiparametric protocols, typically including T1-, T2-, and contrast-enhanced T1-weighted sequences 52,53. Preprocessing consistently incorporated bias-field correction, intensity normalisation, and voxel-size harmonisation to mitigate scanner- and acquisition-related variability 52,53. Feature extraction largely followed standardised, handcrafted radiomic workflows aligned with IBSI definitions, while some recent studies additionally integrated DL-based representations 52. Feature selection commonly relied on regularisation-based or filter methods, such as LASSO, whereas predictive modelling employed logistic regression, support vector machines, or hybrid machine learning (ML) – DL architectures 52,53. Notably, MRI-based investigations placed greater emphasis on feature reproducibility, frequently quantified using intraclass correlation coefficients, reflecting the inherent variability of MRI signal intensities 52,53.
PET-CT-based studies, although fewer in number, generally reported well-structured and methodologically consistent workflows. Tumour segmentation was commonly performed using semi-automatic approaches, including gradient-based algorithms or standardised uptake value (SUV) –based thresholding strategies to delineate metabolically active tumour volumes, often followed by visual inspection and manual refinement 54,55. Preprocessing typically involved voxel-size standardisation and intensity discretisation, and in multi-scanner settings also included harmonisation procedures, reflecting the quantitative nature of PET signal acquisition 54-56. Extracted features comprised SUV-derived metrics, metabolic volume-related parameters, and three-dimensional texture descriptors 56. Feature selection strategies included regularisation-based methods such as LASSO as well as alternative feature-ranking approaches, while predictive modelling relied on ML classifiers-including support vector machines and random forests or survival -oriented models, primarily for prognostic stratification 54-56. As with CT and MRI radiomics, validation in PET-CT studies remained predominantly internal, most commonly using cross-validation or internal split-sample approaches.
Overall, the available literature highlights a predominance of radiomic pipelines based on handcrafted features, a progressive integration of DL methodologies in both feature extraction and modelling phases, and substantial variability in segmentation procedures, feature stability assessments, and validation strategies.
T category assessment
Radiomics has demonstrated a significant contribution to improving the accuracy of T staging in laryngeal cancer, particularly in overcoming the limitations of conventional imaging for assessing cartilage invasion. One of the earliest systematic investigations was conducted by Wang et al. 57, who developed a CT-based radiomic nomogram to improve discrimination between T categories. In a retrospective cohort of 211 patients with LSCC, more than 1300 radiomic features were extracted from preoperative CT scans and subsequently reduced through reproducibility testing and LASSO-based feature selection. The radiomic signature alone achieved an Area Under the Curve (AUC) of 0.850 in the training cohort and 0.862 in the validation cohort, outperforming T staging based on radiologists’ assessment (AUC 0.751 and 0.775, respectively). Importantly, the combined radiomic nomogram integrating the radiomic signature with radiologist-reported T category further improved diagnostic performance, reaching an AUC of 0.899 in the training set and 0.892 in the validation cohort. This approach showed superior capability in distinguishing T3 from T4 tumours, a well-recognised diagnostic challenge in the presence of inflammatory changes, incomplete cartilage ossification, or extra-laryngeal extension.
Consistent with these findings, Guo et al. 58 investigated the prediction of thyroid cartilage invasion in patients with laryngeal and hypopharyngeal SCC, a key determinant for distinguishing T3 from T4 disease. Radiomics-based models, including logistic regression and logistic regression combined with support vector machine-based synthetic minority oversampling, achieved higher AUC values (0.876 and 0.905, respectively) than radiologist assessment (AUC 0.721). These results indicate that CT-based radiomic features can improve the detection of thyroid cartilage invasion compared with conventional visual assessment.
More recent developments have integrated DL techniques, combining handcrafted radiomic features with CNN-derived representations. Chen et al. 59 developed a hybrid CT-based model to distinguish early-stage (I-II) from advanced-stage (III-IV) disease in a cohort of 319 patients. In the test set, the combined model achieved an AUC of 0.849, outperforming both pure radiomics (0.704) and standalone DL (0.724). Gradient-weighted Class Activation Mapping (Grad-CAM) was used to visualise model attention, suggesting a focus on tumour-related regions. Overall, these results support the complementary value of integrating radiomics and DL features, which capture different and potentially synergistic aspects of tumour phenotype.
Adding to this evidence, Xie et al. 52 extended this approach to multiparametric MRI in a multicentre setting. In a cohort of 401 patients, the authors developed radiomics-based, DL-based, and integrated models for preoperative T-category classification. The integrated model achieved the best performance, with an AUC of 0.913 in the internal test set and 0.877 in the external validation cohort, significantly outperforming expert radiologists (AUC ≈ 0.71). Interpretability analyses using SHapley Additive exPlanations (SHAP) and Grad-CAM illustrated that radiomic features and DL contributed complementary information to the model’s predictions, supporting the added value of their integration.
N category assessment
Recently, increasing interest has focused on the application of radiomics for preoperative N category assessment in LSCC. Liang et al. 60 developed a multimodal nomogram integrating clinical imaging features, handcrafted radiomic features, and CT-derived DL radiomics in a cohort of 235 patients. The combined DL-radiomics (DLR) nomogram achieved excellent performance in discriminating nodal metastatic status, with AUCs of 0.934 in the training set and 0.864 in the validation set, outperforming models based on clinical imaging features, conventional radiomics, or DLR alone. Notably, the proposed approach demonstrated improved accuracy over conventional CT morphologic criteria commonly used for nodal staging.
Prognostic applications
Radiomics has been also investigated as a prognostic tool in LSCC. In the CT setting, Chen et al. 43 demonstrated that a preoperatively extracted radiomics signature predicted overall survival (OS), achieving C-indices of 0.78 in the training cohort and 0.75 in the validation cohort. The integration of radiomic features with clinical variables into a radiomics nomogram further improved prognostic performance, yielding C-indices of 0.82 and 0.91 in the training and validation cohorts, respectively.
Qi et al. 46 evaluated the prognostic relevance of CT-based radiomics-derived immunophenotyping in LSCC, comparing whole-tumour and habitat-based approaches. In the testing cohort, the whole-tumour model using logistic regression achieved higher discriminative performance for immunophenotype classification than the habitat-based K-Nearest Neighbors (KNN) model (AUC 0.741 vs 0.611), although the difference was not statistically significant (p = 0.112). Importantly, multivariable Cox regression analysis demonstrated that radiomics-predicted immunophenotyping derived from the optimal model was an independent predictor of unfavorable disease-free survival (DFS) (p = 0.009) and OS (p = 0.008) in patients affected by LSCC.
Integrated DLR models have also been applied for prognostic assessment. Jiang et al. 48 reported that a hybrid CT-based DLR model achieved strong prognostic performance for recurrence-free survival (RFS), with a C-index up to 0.83 and time-dependent AUCs reaching ~0.89 (3-year AUC in the training cohort). Similarly, Chen et al. 50 developed a contrast-enhanced CT-based DLR framework initially designed for local invasion assessment; however, the derived DL signature was independently associated with DFS, supporting its prognostic relevance.
Within the PET-CT domain, Nakajo et al. 56 showed that combining metabolic and textural radiomic features can enhance prognostic modelling. A Naïve Bayes classifier achieved AUCs of approximately 0.81-0.84 for progression prediction, while a Random Survival Forest model reached C-indices of about 0.81-0.84 for progression-free survival (PFS) estimation.
Using a pre-post treatment PET-CT radiomics framework, Choi et al. 55 demonstrated that radiomic features were independently associated with both PFS (p = 0.024) and OS (p = 0.009). The combined clinical-radiomic models achieved robust discrimination, with C-indices for PFS and OS reaching approximately 0.80-0.89 and 0.86-0.96, respectively.
Discussion
Recent literature indicates that radiomics is progressively emerging as a promising tool in the characterisation of LSCC, contributing to advances in preoperative staging, prognostic stratification, and treatment planning. By enabling the extraction of quantitative descriptors from CT, MRI, and PET-CT images, radiomics helps address key limitations of conventional imaging, which relies primarily on qualitative assessment and is subject to inter- and intra-observer variability. The integration of AI methods further enhances this capability by enabling the analysis of morphological, intensity-based, and textural patterns that may not be readily captured by visual assessment alone, thereby offering complementary information related to tumour heterogeneity and underlying biological characteristics 52,61.
Several early studies, including that by Wang et al. 57, demonstrated that radiomics can improve discrimination among clinically relevant T categories, particularly between T3 and T4 tumours, where assessment of cartilage invasion remains challenging. Consistent findings were reported by Guo et al. 58, who developed a CT-based radiomic model for predicting thyroid cartilage invasion that significantly outperformed expert visual assessment. These results highlight the potential of radiomics to provide complementary quantitative information beyond conventional imaging evaluation, potentially reducing diagnostic uncertainty in the assessment of cartilage involvement.
Building on this line of research, Chen et al. 50 further explored CT-based DL approaches and demonstrated that DL-derived models, particularly 2D architectures, achieved superior and more stable performance than handcrafted radiomics models and expert readers in predicting thyroid cartilage invasion, underscoring the ability of DL to learn high-level imaging representations beyond manually engineered features.
This synergistic effect was further confirmed in the multicentre MRI study by Xie et al. 52, in which an integrated radiomics-DL model surpassed both unimodal approaches and the diagnostic performance of experienced radiologists. Together, these studies indicate that DL is particularly effective in capturing complex tumour morphology, while radiomics provides structured and reproducible measures of intratumoural heterogeneity.
Increasing attention has also been directed toward nodal staging. Liang et al. 60 developed an integrated nomogram incorporating clinical variables, radiomic features, and DL-derived information, demonstrating superior performance compared with conventional morphology-based CT criteria for predicting lymph node metastasis. These findings suggest that radiomics-based approaches may improve nodal assessment beyond size-based and structural criteria, with potential implications for surgical planning and radiotherapy target delineation.
In the prognostic domain, 18F-FDG PET-CT-based radiomics has shown encouraging results. Choi et al. 55 demonstrated that radiomics features extracted from longitudinal pre- and post-treatment PET-CT examinations were significantly associated with PFS and OS, and improved prognostic stratification when integrated with clinical variables. Similarly, Nakajo et al. 56 demonstrated that ML-based analysis of pretreatment 18F-FDG PET radiomic features provided robust prognostic stratification for disease progression, highlighting the value of PET-derived textural heterogeneity in outcome prediction.
Complementary CT-based studies further support the clinical relevance of radiomics. Kang et al. 51 demonstrated that CT-derived radiomic features were significantly associated with pathological response to induction chemotherapy in locally advanced LSCC, with the resulting radiomic signature also showing prognostic value for OS, while Chen et al. 43 developed a CT-based radiomic nomogram that demonstrated significantly superior prognostic performance compared with conventional AJCC/TNM staging.
Despite these encouraging findings, several challenges continue to limit the clinical translation of radiomics. Most published studies remain retrospective and single centre, often with relatively small cohorts, increasing the risk of overfitting and restricting generalisability. Moreover, substantial heterogeneity in imaging acquisition, segmentation approaches, feature extraction pipelines, and modeling strategies has led to inconsistent identification and limited reproducibility of predictive radiomic signatures across studies 62-67. Although the IBSI has proposed harmonisation guidelines, their widespread adoption remains limited.
The lack of external validation remains an additional barrier, because validation is often restricted to internal split-sample cohorts and/or small validation sets, while truly independent external testing is inconsistently performed, limiting robustness and reproducibility of proposed models 43,55,60,63.
Despite their promising predictive performance, the deployment of ML and DL models in clinical practice remains challenging. Emerging methodologies may help address these limitations. Federated learning offers a potential framework for developing robust, multi-institutional radiomic models while preserving data privacy 68.
In summary, current evidence supports the potential role of radiomics as a valuable adjunct for staging, prognostic assessment, and treatment planning in LSCC, enabling quantitative characterisation of tumour heterogeneity beyond conventional imaging. However, widespread clinical adoption will require standardised imaging protocols, prospective multicentre validation, and improved interpretability of advanced analytical models to ensure reliability and clinical trust.
Conclusions
Radiomics is an emerging tool in the evaluation of LSCC, with promising applications in staging, prognostic assessment, and prediction of treatment response. Models integrating radiomic features with DL and clinical variables have shown improved performance compared with conventional imaging in selected settings, suggesting added value in capturing tumour heterogeneity. However, routine clinical adoption remains limited by methodological variability, small single-centre cohorts, lack of external validation, and the limited interpretability of advanced algorithms. Progress in standardisation, multicentre prospective studies, and explainable AI will be essential to ensure reproducibility and clinical reliability.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
SL, AV: conceptualization, literature search; SL: writing original draft; SL, FL, GP: writing, review and editing; AV: supervision.
All authors have read and approved the final version of the manuscript.
Ethical consideration
Not applicable.
History
Received: February 2, 2026
Accepted: February 4, 2026
Figures and tables
| Author/year | Model | AUC/C-index training | AUC/C-index validation | Conclusion |
|---|---|---|---|---|
| Chen et al., 2020 43 | Radiomics signature | C-index ~ 0.78 | C-index ~ 0.75 | Radiomics improved OS/PFS prediction vs clinical model |
| Clinical nomogram | C-index ~ 0.80 | C-index ~ 0.81 | ||
| Radiomics nomogram | C-index ~ 0.82 | C-index ~ 0.91 | ||
| Rajgor et al., 2024 44 | Clinical-only model | C-index ~ 0.65 | - | Radiomics independently predicted survival |
| Combined model | C-index ~ 0.76 | - | ||
| Qi et al., 2024 46 | Radiomics from whole-tumour | AUC ~ 0.82 (KNN) | AUC ~ 0.70 (KNN) | Whole-tumour radiomics improved prediction of immunophenotype |
| AUC ~ 0.80 (NB) | AUC ~ 0.72 (NB) | |||
| AUC ~ 0.78 (LR) | AUC ~ 0.74 (LR) | |||
| Radiomics from habitat region | AUC ~ 0.86 (KNN) | AUC ~ 0.61 (KNN) | ||
| AUC ~ 0.76 (NB) | AUC ~ 0.61 (NB) | |||
| AUC ~ 0.74 (LR) | AUC ~ 0.61 (LR) | |||
| Dong et al., 2025 47 | Habitat radiomics nomogram | AUC ~ 0.80 | AUC ~ 0.77 | HI radiomics improved prediction of Ki-67 positivity |
| Jiang et al., 2025 48 | Clinical | C-index ~ 0.68 | C-indexint ~ 0.63 | Improved survival prediction |
| C-indexext ~ 0.60 | ||||
| RS | C-index ~ 0.71 | C-indexint ~ 0.68 | ||
| C-indexext ~ 0.62 | ||||
| DLS | C-index ~ 0.74 | C-indexint ~ 0.73 | ||
| C-indexext ~ 0.73 | ||||
| Hybrid RS-DLS | C-index ~ 0.83 | C-indexint ~ 0.81 | ||
| C-indexext ~ 0.74 | ||||
| Ma et al., 2025 49 | Clinical | C-index ~ 0.76 | C-indexext ~ 0.60 | Multi-channel deep learning radiomics model showed promising performance for predicting OS |
| Radiomics | C-index ~ 0.84 | C-indexext ~ 0.73 | ||
| Deep learning | C-index ~ 0.85 | C-indexext ~ 0.72 | ||
| Deep learning radiomics nomogram | C-index ~ 0.90 | C-indexext ~ 0.73 | ||
| Kang et al., 2023 51 | Clinico-pathological + radiomics | C-index ~ 0.80 | C-index ~ 0.74 | Predicted PR and OS |
| Wang et al., 2019 57 | Radiologist performance | AUC ~ 0.77 | AUC ~ 0.78 | Improved preoperative T staging accuracy |
| Radiomics | AUC ~ 0.86 | AUC ~ 0.77 | ||
| Combined | AUC ~ 0.89 | AUC ~ 0.78 | ||
| Guo et al., 2020 58 | Radiologist | AUC ~ 0.72 | - | Improved prediction of cartilage invasion |
| Radiomic LR | AUC ~ 0.88 | - | ||
| Radiomic LR-SVM SMOTE | AUC ~ 0.90 | - | ||
| Xie et al., 2025 52 | Radiologist | AUC ~ 0.72 | AUCext ~ 0.71 | Improved stage disease discrimination (I-II vs III-IV) |
| Radiomics | AUC ~ 0.86 | AUCext ~ 0.84 | ||
| Deep learning | AUC ~ 0.82 | AUCext ~ 0.81 | ||
| Deep learning + radiomics | AUC ~ 0.91 | AUCext ~ 0.88 | ||
| Zhong et al., 2021 54 | PET | AUC ~ 0.91 | AUC ~ 0.82 | Improved outcome prediction |
| CT | AUC ~ 0.94 | AUC ~ 0.72 | ||
| Clinical | AUC ~ 0.88 | AUC ~ 0.70 | ||
| PET+CT | AUC ~ 0.93 | AUC ~ 0.94 | ||
| Choi et al., 2024 55 | Clinical | C-index ~ 0.76 | C-index ~ 0.89 | Combined features predicted PFS better than SUV metrics |
| Clinical + radiomics | C-index ~ 0.80 | C-index ~ 0.89 | ||
| Clinical | C-index ~ 0.80 | C-index ~ 0.92 | Combined features predicted OS better than SUV metrics | |
| Clinical + radiomics | C-index ~ 0.86 | C-index ~ 0.96 | ||
| Nakajo et al., 2023 56 | PET radiomics | AUC ~ 0.81 | AUC ~ 0.84 | Improved prognostic prediction |
| Liang et al., 2025 60 | Clinical imaging | AUC ~ 0.83 | AUC ~ 0.82 | Accurate LNM prediction |
| Conventional radiomics | AUC ~ 0.86 | AUC ~ 0.82 | ||
| Deep learning radiomics | AUC ~ 0.91 | AUC ~ 0.83 | ||
| DL-radiomics nomogram | AUC ~ 0.93 | AUC ~ 0.86 | ||
| AUC: area under the curve; CT: computed tomography; DLS: deep learning score; HI: habitat imaging; KNN: K nearest neighbor; LNM: lymph node metastasis; LR: logistic regression; NB: naïve bayes; OS: overall survival; PET: positron emission tomography; PFS: progression free survival; PR: pathological response; RS: radiomic score; SMOTE: synthetic minority over-sampling technique; SUV: standard uptake value; SVM: support vector machine. | ||||
| Author/year | No. of patients | Study type | Imaging modality | Segmentation | Radiomics/model development |
|---|---|---|---|---|---|
| Chen et al., 2020 43 | 136 | Retrospective | CT | Manual 3D ROI | Handcrafted radiomics; LASSO-Cox |
| Qi et al., 2024 46 | 106 | Retrospective | CT | Manual 3D + habitat segmentation | Handcrafted + wavelet; ML classifiers |
| Dong et al., 2025 47 | 128 | Retrospective | CT (dual-energy) | Manual 3D + K-means habitats | Handcrafted + wavelet; ML + nomogram |
| Jiang et al., 2025 48 | 349 (Centre 1) | Retrospective multicentre | CT | Manual 3D VOI | Radiomics + CNN; cox models |
| 78 (Centre 2) | |||||
| Ma et al., 2025 49 | 156 (Centre 1) | Retrospective multicentre | CT | Manual 3D VOI | Radiomics + DL features; cox nomogram |
| 116 (Centre 2) | |||||
| Kang et al., 2023 51 | 114 | Retrospective | CT | Manual ROI | Handcrafted radiomics; LASSO + regression |
| Xie et al., 2025 52 | 401 (Centre 1-2) | Retrospective multicentre | MRI | Manual 3D VOI | Radiomics + DL; random forest |
| Chen et al., 2024 53 | 351 (Centre 1-2) | Retrospective multicentre | MRI | Manual 3D VOI | Radiomics; ML classifiers + nomogram |
| Zong et al., 2021 54 | 72 | Retrospective | PET/CT | Semi-automatic SUV-threshold + manual | Radiomics; random forest |
| Choi et al., 2024 55 | 91 | Retrospective | PET/CT | Gradient-based semi-automatic | Radiomics; LASSO + survival models |
| Nakajo et al., 2023 56 | 100 | Retrospective | PET/CT | SUV-threshold VOI | Radiomics; ML + survival ML |
| CNN: convolutional neural network; CT: computed tomography; DL: deep learning; LASSO: least absolute shrinkage and selection operator; ML: machine learning; PET: positron emission tomography; ROI: region of interest; SUV: standard uptake value; VOI: volume of interest. | |||||
References
- Mody M, Rocco J, Yom S. Head and neck cancer. Lancet. 2021;398:2289-2299. doi:https://doi.org/10.1016/S0140-6736(21)01550-6
- Bray F, Laversanne M, Sung H. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229-263. doi:https://doi.org/10.3322/caac.21834
- Ciolofan M, Vlăescu A, Mogoantă C. Clinical, histological and immunohistochemical evaluation of larynx cancer. Curr Health Sci J. 2017;43:367-375. doi:https://doi.org/10.12865/CHSJ.43.04.14
- Chang C, Chang S, Chuang S. Age at start of using tobacco on the risk of head and neck cancer: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium (INHANCE). Cancer Epidemiol. 2019;63. doi:https://doi.org/10.1016/j.canep.2019.101615
- Di Credico G, Edefonti V, Polesel J. Joint effects of intensity and duration of cigarette smoking on the risk of head and neck cancer: a bivariate spline model approach. Oral Oncol. 2019;94:47-57. doi:https://doi.org/10.1016/j.oraloncology.2019.05.006
- Hut A, Boia E, Para D. Laryngeal cancer in the modern era: evolving trends in diagnosis, treatment, and survival outcomes. J Clin Med. 2025;14. doi:https://doi.org/10.3390/jcm14103367
- Crosetti E, Pilolli F, Succo G. A new strategy for endoscopic staging of laryngeal carcinoma: multistep endoscopy. Acta Otorhinolaryngol Ital. 2012;32:175-181.
- De Vito A, Meccariello G, Vicini C. Narrow band imaging as screening test for early detection of laryngeal cancer: a prospective study. Clin Otolaryngol. 2017;42:347-353. doi:https://doi.org/10.1111/coa.12728
- Gupta T, Master Z, Kannan S. Diagnostic performance of post-treatment FDG PET or FDG PET/CT imaging in head and neck cancer: a systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. 2011;38:2083-2095. doi:https://doi.org/10.1007/s00259-011-1893-y
- Sarkar A, Sharma N, Raghavan A. Role of computed tomography, magnetic resonance imaging, and endoscopy in pretherapeutic evaluation of laryngeal tumors. Astrocyte. 2016;2. doi:https://doi.org/10.4103/2349-0977.191045
- Preda L, Conte G, Bonello L. Diagnostic accuracy of surface coil MRI in assessing cartilaginous invasion in laryngeal tumours: do we need contrast-agent administration?. Eur Radiol. 2017;27:4690-4698. doi:https://doi.org/10.1007/s00330-017-4840-x
- Itamura K, Hsue V, Barbu A. Diagnostic assessment (imaging) and staging of laryngeal cancer. Otolaryngol Clin North Am. 2023;56:215-231. doi:https://doi.org/10.1016/j.otc.2022.12.006
- Contrera K, Hair B, Prendes B. Clinical versus pathologic laryngeal cancer staging and the impact of stage change on outcomes. Laryngoscope. 2021;131:559-565. doi:https://doi.org/10.1002/lary.28924
- Chiesa-Estomba C, Echaniz O, Larruscain E. Radiomics and texture analysis in laryngeal cancer. Looking for new frontiers in precision medicine through imaging analysis. Cancers (Basel). 2019;11. doi:https://doi.org/10.3390/cancers11101409
- Scheckenbach K. Radiomics: big data instead of biopsies in the future?. Laryngorhinootologie. 2018;97:S114-S141. doi:https://doi.org/10.1055/s-0043-121964
- Ulrich E, Menda Y, Boles Ponto L. FLT PET radiomics for response prediction to chemoradiation therapy in head and neck squamous cell cancer. Tomography. 2019;5:161-169. doi:https://doi.org/10.18383/j.tom.2018.00038
- Guezennec C, Robin P, Orlhac F. Prognostic value of textural indices extracted from pretherapeutic 18-F FDG-PET/CT in head and neck squamous cell carcinoma. Head Neck. 2019;41:495-502. doi:https://doi.org/10.1002/hed.25433
- Aerts H, Velazquez E, Leijenaar R. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat Commun. 2014;5. doi:https://doi.org/10.1038/ncomms5006
- Alic L, Niessen W, Veenland J. Quantification of heterogeneity as a biomarker in tumor imaging: a systematic review. PLoS One. 2014;9. doi:https://doi.org/10.1371/journal.pone.0110300
- Carvalho S, Leijenaar R, Velazquez E. Prognostic value of metabolic metrics extracted from baseline positron emission tomography images in non-small cell lung cancer. Acta Oncol. 2013;52:1398-1404. doi:https://doi.org/10.3109/0284186X.2013.812795
- Gevaert O, Mitchell L, Achrol A. Glioblastoma multiforme: exploratory radiogenomic analysis by using quantitative image features. Radiology. 2014;273:168-174. doi:https://doi.org/10.1148/radiol.14131731
- Hatt M, Tixier F, Cheze Le Rest C. Robustness of intratumour 18F-FDG PET uptake heterogeneity quantification for therapy response prediction in oesophageal carcinoma. Eur J Nucl Med Mol Imaging. 2013;40:1662-1671. doi:https://doi.org/10.1007/s00259-013-2486-8
- Jain R, Poisson L, Gutman D. Outcome prediction in patients with glioblastoma by using imaging, clinical, and genomic biomarkers: focus on the nonenhancing component of the tumor. Radiology. 2014;272:484-493. doi:https://doi.org/10.1148/radiol.14131691
- Leijenaar R, Carvalho S, Velazquez E. Stability of FDG-PET radiomics features: an integrated analysis of test-retest and inter-observer variability. Acta Oncol. 2013;52:1391-1397. doi:https://doi.org/10.3109/0284186X.2013.812798
- Parmar C, Rios Velazquez E, Leijenaar R. Robust radiomics feature quantification using semiautomatic volumetric segmentation. PLoS One. 2014;9. doi:https://doi.org/10.1371/journal.pone.0102107
- Hunter L, Krafft S, Stingo F. High quality machine-robust image features: identification in nonsmall cell lung cancer computed tomography images. Med Phys. 2013;40. doi:https://doi.org/10.1118/1.4829514
- Parmar C, Leijenaar R, Grossmann P. Radiomic feature clusters and prognostic signatures specific for lung and head and neck cancer. Sci Rep. 2015;5. doi:https://doi.org/10.1038/srep11044
- Ganeshan B, Goh V, Mandeville H. Non-small cell lung cancer: histopathologic correlates for texture parameters at CT. Radiology. 2013;266:326-336. doi:https://doi.org/10.1148/radiol.12112428
- Segal E, Sirlin C, Ooi C. Decoding global gene expression programs in liver cancer by noninvasive imaging. Nat Biotechnol. 2007;25:675-680. doi:https://doi.org/10.1038/nbt1306
- Nicolasjilwan M, Hu Y, Yan C. Addition of MR imaging features and genetic biomarkers strengthens glioblastoma survival prediction in TCGA patients. J Neuroradiol. 2015;42:212-221. doi:https://doi.org/10.1016/j.neurad.2014.02.006
- Traverso A, Wee L, Dekker A. Repeatability and reproducibility of radiomic features: a systematic review. Int J Radiat Oncol Biol Phys. 2018;102:1143-1158. doi:https://doi.org/10.1016/j.ijrobp.2018.05.053
- Lambin P, Leijenaar R, Deist T. Radiomics: the bridge between medical imaging and personalized medicine. Nat Rev Clin Oncol. 2017;14:749-762. doi:https://doi.org/10.1038/nrclinonc.2017.141
- Shur J, Doran S, Kumar S. Radiomics in oncology: a practical guide. Radiographics. 2021;41:1717-1732. doi:https://doi.org/10.1148/rg.2021210037
- Ellingson B, Zaw T, Cloughesy T. Comparison between intensity normalization techniques for dynamic susceptibility contrast (DSC)-MRI estimates of cerebral blood volume (CBV) in human gliomas. J Magn Reson Imaging. 2012;35:1472-1477.
- Vovk U, Pernus F, Likar B. A review of methods for correction of intensity inhomogeneity in MRI. IEEE Trans Med Imaging. 2007;26:405-421. doi:https://doi.org/10.1109/TMI.2006.891486
- Shafiq-Ul-Hassan M, Zhang G, Latifi K. Intrinsic dependencies of CT radiomic features on voxel size and number of gray levels. Med Phys. 2017;44:1050-1062. doi:https://doi.org/10.1002/mp.12123
- Zwanenburg A, Vallières M, Abdalah M. The Image Biomarker Standardization Initiative: standardized quantitative radiomics for high-throughput image-based phenotyping. Radiology. 2020;295:328-338. doi:https://doi.org/10.1148/radiol.2020191145
- Napel S, Mu W, Jardim-Perassi B. Quantitative imaging of cancer in the postgenomic era: radio(geno)mics, deep learning, and habitats. Cancer. 2018;124:4633-4649. doi:https://doi.org/10.1002/cncr.31630
- Beig N, Khorrami M, Alilou M. Perinodular and intranodular radiomic features on lung CT images distinguish adenocarcinomas from granulomas. Radiology. 2019;290:783-792. doi:https://doi.org/10.1148/radiol.2018180910
- Zwanenburg A, Leger S, Agolli L. Assessing robustness of radiomic features by image perturbation. Sci Rep. 2019;9. doi:https://doi.org/10.1038/s41598-018-36938-4
- McHugh D, Porta N, Little R. Image contrast, image pre-processing, and T1 mapping affect MRI radiomic feature repeatability in patients with colorectal cancer liver metastases. Cancers (Basel). 2021;13. doi:https://doi.org/10.3390/cancers13020240
- Fornacon-Wood I, Mistry H, Ackermann C. Reliability and prognostic value of radiomic features are highly dependent on choice of feature extraction platform. Eur Radiol. 2020;30:6241-6250. doi:https://doi.org/10.1007/s00330-020-06957-9
- Chen L, Wang H, Zeng H. Evaluation of CT-based radiomics signature and nomogram as prognostic markers in patients with laryngeal squamous cell carcinoma. Cancer Imaging. 2020;20. doi:https://doi.org/10.1186/s40644-020-00310-5
- Rajgor A, Kui C, McQueen A. Computed tomography-based radiomic markers are independent prognosticators of survival in advanced laryngeal cancer: a pilot study. J Laryngol Otol. 2024;138:685-691. doi:https://doi.org/10.1017/S0022215123002372
- Cui F, Khodrog O, Liu W. Clinical application of CT-based radiomics model in differentiation between laryngeal squamous cell carcinoma and squamous cell hyperplasia. Front Med (Lausanne). 2024;10. doi:https://doi.org/10.3389/fmed.2023.1337723
- Qi M, Zhou W, Yuan Y. Computed tomography radiomics reveals prognostic value of immunophenotyping in laryngeal squamous cell carcinoma: a comparison of whole tumor- versus habitats-based approaches. BMC Med Imaging. 2024;24. doi:https://doi.org/10.1186/s12880-024-01491-2
- Dong Y, Yang S, Jing X. Habitat imaging radiomics increases the accuracy of a nomogram for predicting Ki-67-positivity in laryngeal squamous cell carcinoma. Eur J Radiol Open. 2025;14. doi:https://doi.org/10.1016/j.ejro.2025.100659
- Jiang H, Xie K, Chen X. A prognostic model integrating radiomics and deep learning based on CT for survival prediction in laryngeal squamous cell carcinoma. Sci Rep. 2025;15. doi:https://doi.org/10.1038/s41598-025-15166-7
- Ma H, Wei W, Zhang J. Multi-channel deep learning radiomics model based on contrast-enhanced CT for predicting postoperative prognosis in laryngeal carcinoma. BMC Cancer. 2025;25. doi:https://doi.org/10.1186/s12885-025-14912-4
- Chen X, Xia S, Jiang H. CT-based radiomics and deep learning models for predicting thyroid cartilage invasion and patient prognosis in laryngeal carcinoma. Sci Rep. 2025;15. doi:https://doi.org/10.1038/s41598-025-23809-y
- Kang C, Sun P, Yang R. CT radiomics nomogram predicts pathological response after induced chemotherapy and overall survival in patients with advanced laryngeal cancer: a single-center retrospective study. Front Oncol. 2023;13. doi:https://doi.org/10.3389/fonc.2023.1094768
- Xie K, Jiang H, Chen X. Multiparameter MRI-based model integrating radiomics and deep learning for preoperative staging of laryngeal squamous cell carcinoma. Sci Rep. 2025;15. doi:https://doi.org/10.1038/s41598-025-01270-1
- Chen W, Lin G, Chen Y. Prediction of the Ki-67 expression level in head and neck squamous cell carcinoma with machine learning-based multiparametric MRI radiomics: a multicenter study. BMC Cancer. 2024;24. doi:https://doi.org/10.1186/s12885-024-12026-x
- Zhong J, Frood R, Brown P. Machine learning-based FDG PET-CT radiomics for outcome prediction in larynx and hypopharynx squamous cell carcinoma. Clin Radiol. 2021;76:78.e9-78.e17. doi:https://doi.org/10.1016/j.crad.2020.08.030
- Choi J, Choi J, Woo S. Prognostic value of radiomic analysis using pre- and post-treatment 18F-FDG-PET/CT in patients with laryngeal cancer and hypopharyngeal cancer. J Pers Med. 2024;14. doi:https://doi.org/10.3390/jpm14010071
- Nakajo M, Nagano H, Jinguji M. The usefulness of machine-learning-based evaluation of clinical and pretreatment 18F-FDG-PET/CT radiomic features for predicting prognosis in patients with laryngeal cancer. Br J Radiol. 2023;96. doi:https://doi.org/10.1259/bjr.20220772
- Wang F, Zhang B, Wu X. Radiomic nomogram improves preoperative T category accuracy in locally advanced laryngeal carcinoma. Front Oncol. 2019;9. doi:https://doi.org/10.3389/fonc.2019.01064
- Guo R, Guo J, Zhang L. CT-based radiomics features in the prediction of thyroid cartilage invasion from laryngeal and hypopharyngeal squamous cell carcinoma. Cancer Imaging. 2020;20. doi:https://doi.org/10.1186/s40644-020-00359-2
- Chen X, Yu Q, Peng J. A combined model integrating radiomics and deep learning based on contrast-enhanced CT for preoperative staging of laryngeal carcinoma. Acad Radiol. 2023;30:3022-3031. doi:https://doi.org/10.1016/j.acra.2023.06.029
- Liang Y, He M, Chen W. Deep learning radiomics nomogram predicts lymph node metastasis in laryngeal squamous cell carcinoma. Front Oncol. 2025;15. doi:https://doi.org/10.3389/fonc.2025.1573687
- Lambin P, Rios-Velazquez E, Leijenaar R. Radiomics: extracting more information from medical images using advanced feature analysis. Eur J Cancer. 2012;48:441-446. doi:https://doi.org/10.1016/j.ejca.2011.11.036
- Cozzi L, Franzese C, Fogliata A. Predicting survival and local control after radiochemotherapy in locally advanced head and neck cancer by means of computed tomography based radiomics. Strahlenther Onkol. 2019;195:805-818. doi:https://doi.org/10.1007/s00066-019-01483-0
- Kuno H, Qureshi M, Chapman M. CT texture analysis potentially predicts local failure in head and neck squamous cell carcinoma treated with chemoradiotherapy. AJNR Am J Neuroradiol. 2017;38:2334-2340. doi:https://doi.org/10.3174/ajnr.A5407
- Rao D, Koteshwara P, Singh R. Exploring radiomics for classification of supraglottic tumors: a pilot study in a tertiary care center. Indian J Otolaryngol Head Neck Surg. 2023;75:433-439. doi:https://doi.org/10.1007/s12070-022-03239-2
- Zhao X, Li W, Zhang J. Radiomics analysis of CT imaging improves preoperative prediction of cervical lymph node metastasis in laryngeal squamous cell carcinoma. Eur Radiol. 2023;33:1121-1131. doi:https://doi.org/10.1007/s00330-022-09051-4
- Masson I, Da-Ano R, Lucia F. Statistical harmonization can improve the development of a multicenter CT-based radiomic model predictive of nonresponse to induction chemotherapy in laryngeal cancers. Med Phys. 2021;48:4099-4109. doi:https://doi.org/10.1002/mp.14948
- Agarwal J, Sinha S, Goda J. Tumor radiomic features complement clinico-radiological factors in predicting long-term local control and laryngectomy free survival in locally advanced laryngo-pharyngeal cancers. Br J Radiol. 2020;93. doi:https://doi.org/10.1259/bjr.20190857
- Raza A, Guzzo A, Ianni M. Federated learning in radiomics: a comprehensive meta-survey on medical image analysis. Comput Methods Programs Biomed. 2025;267. doi:https://doi.org/10.1016/j.cmpb.2025.108768
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 464 times
- PDF downloaded - 128 times