Annual congress report
Vol. 46: 112 TH CONGRESS SIOECHCF - OFFICIAL REPORT 2026
Systemic therapy in the curative treatment of laryngeal cancer
Summary
Cover Image
The aim of this narrative review is to provide a comprehensive overview of systemic approaches in the context of curative treatments for laryngeal squamous cell carcinoma, evaluating oncologic outcomes, survival, and the preservation of voice and swallowing functions. It summarises current evidence from landmark clinical trials, international guidelines, and recent developments in multidisciplinary management, including systemic therapies and advanced radiation techniques. Early-stage laryngeal SCC shows high rates of cure with either surgery or radiotherapy. For locally advanced disease, concurrent chemoradiation remains the nonsurgical standard for organ preservation, though it offers no significant survival advantage over primary surgery. Patient selection is critical; individuals with T4 disease or severe baseline dysfunction often achieve better outcomes with total laryngectomy. While induction chemotherapy and immunotherapy have shown mixed results in definitive settings, neoadjuvant immunotherapy is emerging as a promising approach. Additionally, proton therapy offers potential for reducing late toxicities, such as dysphagia, by better sparing surrounding organs. In conclusion, optimal management of laryngeal cancer requires meticulous multidisciplinary evaluation and personalised treatment. Balancing oncologic control with functional preservation remains the primary challenge, necessitating a shift toward integrated, patient-centred care.
Introduction
Malignant tumours of the head and neck (in particular, head and neck squamous cell carcinomas [HNSCC]) are relatively rare, and patients are generally referred to dedicated centres for HN oncology. In Europe, between 2000 and 2007, the annual crude incidence rates were 4.6/100,000 for laryngeal SCC, 3.5/100,000 for oral cavity SCC, 3.3/100,000 for oropharyngeal SCC, and 1.3/100,000 for hypopharyngeal SCC, corresponding to approximately 90,000 new cases per year 1.
Five-year relative survival rates are 61%, 49%, 41%, and 25% for laryngeal, oral cavity, oropharyngeal, and hypopharyngeal SCC, respectively 2.
Laryngeal SCC accounts for approximately 0.8% of all cancers (up to 2.4% of new malignancies worldwide each year) and is most common in men in the 5th to 7th decades 3.
Laryngeal cancer may involve the supraglottic, glottic, and subglottic regions; the glottic larynx is the most common site 4,5.
More than 95% of laryngeal cancers are SCC 6. Despite numerous advances, 5-year survival has not substantially improved and depends on stage and site. For example, in a Finnish cohort, 5-year disease-specific survivals (DSS) for glottic cancers were 100%, 95%, 78%, 79%, and 53% for T1a, T1b, T2, T3, and T4, respectively; for supraglottic cancers, DSS were 68%, 54%, 72%, and 59% according to T1-T4 categories 7.
Early detection of pathologic tissue changes is crucial for effective treatment and functional preservation. Direct laryngoscopy and biopsy remain the gold standard, while imaging provides essential information for staging, assessment of resectability, prognosis, and treatment planning 8.
In advanced laryngeal cancer (T3-4, N0-3), multimodal treatment is often required. Over the past 150 years, management has shifted from routine radical surgery to more conservative approaches; for early disease, both transoral surgery and primary radiotherapy (RT) are accepted options 9. Systemic therapy (notably, chemotherapy, and, more recently, immunotherapy) plays an important role in advanced disease.
Successful management requires careful pretreatment evaluation of patient- and disease-related factors (Fig. 1), with the dual aim of cure and quality of life preservation, within a multidisciplinary team (MDT) 10,11.
The management of laryngeal cancer (Fig. 2) can be summarised as surgery (including open and transoral approaches), RT, combined chemoradiotherapy (CRT), and, in selected settings, immunotherapy or targeted agents.
Principles of larynx preservation
The goal of this manuscript is to provide an overview of conservative (larynx-preservation) treatment for laryngeal SCC, focusing on survival, locoregional control, response rate, and voice- and swallowing-related quality of life. Priorities for HN patients are reported in Table I.
Larynx-preservation treatment has led to the recommendation that “a function-preserving treatment should be the first choice for every patient with laryngeal carcinoma”, provided that oncologic outcomes are not compromised.
The success of larynx-preservation strategies depends on careful patient and tumour selection. Optimal treatment of advanced disease requires accurate staging and comprehensive evaluation of clinical, behavioral, psychological, socioeconomic, and logistic factors within an MDT.
For early-stage glottic cancer, 3 large systematic reviews have shown comparable high cure rates with either transoral laser/endolaryngeal surgery or RT, confirming that several organ-preserving options are oncologically sound 13-15.
In locally advanced disease (T3-T4), the challenge is to balance survival with long-term functional outcomes. In T3-4, N0-3 disease, multimodal treatment is often needed, and larynx-preservation approaches must not reduce survival compared to total laryngectomy with adjuvant RT.
Baseline assessment of airway, voice, and swallowing is recommended for all patients with stage III/IV disease to guide selection between organ preservation and total laryngectomy and to anticipate the need for feeding or tracheostomy tubes. Patients with large-volume, deeply infiltrative T3/T4a tumours, pretreatment aspiration, cartilage destruction, nonfunctional voice or airway, or severe laryngeal dysfunction are unlikely to have acceptable function after organ-preservation therapies and are generally better served by primary total laryngectomy 16.
Most larynx-preservation series include patients with stage less than IV; poorer results in stage IV have contributed to recommendations for primary surgery – typically total laryngectomy – for T4a disease.
Treatment strategies
General principles
Treatment goals are local tumour control and preservation of laryngeal function. Surgery, RT, chemotherapy, or combinations may be used. Definitive RT, with or without chemotherapy, is a standard option for many early and selected intermediate glottic tumours 17.
Advanced-stage laryngeal cancer encompasses a wide spectrum. Treatment selection should consider tumour extent and subsite (glottic vs supraglottic vs subglottic), vocal cord mobility, anterior commissure involvement, nodal status, patient age, comorbidities, baseline function, preferences, compliance, and local expertise. Lymph node involvement is uncommon in T1-T2 glottic tumours; single-modality treatment directed at the primary is often sufficient.
Key guidelines emphasise that RT alone, open or transoral larynx-preserving surgery, and combined CRT are all acceptable options in selected patients; choice should be individualised 18.
Evidence for concomitant chemo-radiation
For locally advanced HNSCC, CRT with concurrent cisplatin has been the standard for over 2 decades, based on the MACH-NC meta-analyses, which showed an absolute 5-year overall survival (OS) benefit of around 6-7% with concomitant chemotherapy 19-21.
In laryngeal cancer, concurrent CRT offers higher larynx-preservation rates than RT alone or induction chemotherapy followed by RT, at the cost of increased acute toxicity but with no clear OS advantage. Consequently, concurrent cisplatin-based CRT is the preferred nonsurgical larynx-preservation approach in many patients.
Clinical, behavioural, and socioeconomic factors (performance status, nutrition, alcohol use, comorbidities, social support) are key predictors of outcome. The TALK score (T4, albumin < 4 g/dL, ≥6 drinks/day, Karnofsky < 80%) stratifies the probability of successful larynx preservation; only about 6% of patients with scores ≥ 3 ultimately preserve a functional larynx 22. Combined chemotherapy and RT can be used for larynx preservation in selected patients with unfavourable T2 or T2N+ disease when larynx-preserving surgery is not feasible or expected to yield poor function. For stage I-III disease, OS does not clearly differ between surgical and nonsurgical approaches; for stage IV, retrospective data suggest better survival with primary surgery, especially in T4a disease 23,24.
Induction chemotherapy
Induction (i.e., neoadjuvant) chemotherapy followed by RT (or CRT) has been extensively studied as a larynx-preservation strategy in operable T3-T4 laryngeal and hypopharyngeal cancers. The EORTC 24891 hypopharynx trial and EORTC 24954 larynx/hypopharynx trial showed that induction cisplatin-FU (with or without alternating RT) allowed larynx preservation in responders without compromising OS compared with primary surgery plus RT, but did not improve survival 25-27. The addition of a taxane (TPF) increases response and larynx-preservation rates compared with PF doublets, but without OS benefit 28-31.
Nonresponse to induction (≈15% of patients) predicts poor local control and survival despite subsequent RT/CRT and may identify patients who should proceed to early total laryngectomy rather than definitive organ preservation. Induction chemotherapy before organ-preservation surgery is not recommended outside clinical trials.
RTOG 91-11 and role of concurrent CRT
The landmark RTOG 91-11 trial compared RT alone, induction PF followed by RT, and concurrent cisplatin-RT in patients with mostly T3 laryngeal cancer. Concurrent CRT significantly improved larynx-preservation and local control compared with RT alone and with induction PF, but did not improve OS; laryngectomy-free survival (LFS) at 10 years was similar between the 2 chemotherapy arms and worse with RT alone 11,32.
Cisplatin remains the best-supported radiosensitiser. Phase III data for alternative agents (e.g. cetuximab) in larynx-preservation cohorts are limited; a secondary analysis of the Bonner et al. trial suggested a nonsignificant trend toward improved larynx preservation and LFS with cetuximab + RT versus RT alone, but definitive conclusions cannot be drawn 33,34.
Postoperative CRT and selection for total laryngectomy
For patients with extensive T3 or T4a lesions and/or poor pretreatment laryngeal function, primary total laryngectomy followed by RT or CRT often offers better survival and quality of life (QoL) than attempts at organ preservation. Retrospective NCDB analyses confirm that, after adjustment for stage and covariates, RT alone and CRT are associated with worse survival than total laryngectomy in stage IV disease 24. Accurate surgical margins are crucial, as positive or close margins dramatically increase the risk of local recurrence 35.
Among high-risk patients (positive margins and/or extracapsular nodal extension), 2 randomised trials (EORTC 22931 and RTOG 9501) established concurrent postoperative cisplatin-RT as standard of care, improving locoregional control and disease-free survival (DFS) at the cost of increased toxicity 36-38.
Immunotherapy and larynx preservation
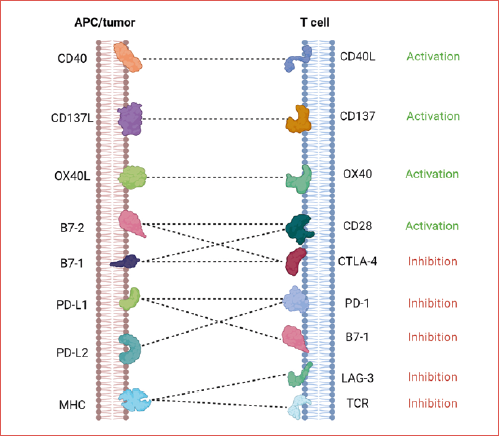
Immunotherapy, notably PD-1/PD-L1 blockade pembrolizumab and nivolumab improve survival compared with standard regimens, particularly in PD-L1-positive disease 39,40 (Cover figure). Checkpoint inhibitors target the PD-1/PD-L1 axis, reversing T-cell exhaustion and restoring antitumour immunity 41. RT has both immunostimulatory and immunosuppressive effects and can synergise with immunotherapy by enhancing antigen release, T-cell infiltration, and MHC-I expression 42,43. The concept of “cancer immunoediting” underscores the dynamic interaction between tumour and immune system 44.
In locally advanced, previously untreated disease, multiple phase II and III trials have evaluated immune checkpoint inhibitors combined with RT or CRT:
- in cisplatin-ineligible patients, RT + pembrolizumab or RT + cetuximab yielded similar locoregional control in PEMBRORAD, with better tolerance in the pembrolizumab arm 45;
- early phase studies of pembrolizumab added to standard CRT showed acceptable safety and high response rates 46;
- large phase III trials (JAVELIN Head and Neck 100 and KEYNOTE-412) testing concurrent and maintenance PD-L1/PD-1 blockade with CRT did not meet their primary endpoints of improved progression-free survival (PFS) or event-free survival, although exploratory analyses suggest possible benefit in highly PD-L1-expressing subgroups 47,48.
In the adjuvant setting, the IMvoke010 trial (atezolizumab after CRT) was negative for OS 49, whereas the NIVOPOSTOP trial showed that adding nivolumab to postoperative CRT in high-risk resected HNSCC significantly improved DFS, representing the first positive phase III escalation of standard CRT in this context 50.
Overall, current evidence indicates that adding immunotherapy to definitive RT or CRT for unselected, locally advanced HNSCC has not yet translated into consistent survival gains, although it may be an attractive option for cisplatin-unfit patients and in the adjuvant high-risk setting.
The most encouraging data come from neoadjuvant strategies. The CheckRad-CD8 phase II trial showed that double checkpoint blockade plus a short induction phase followed by RT was feasible and associated with promising activity 51.
In a multicentre phase II trial, one cycle of neoadjuvant pembrolizumab administered 2-3 weeks before surgery resulted in major pathological responses or extensive tumour necrosis in a substantial proportion of patients 52.
KEYNOTE-689, a phase III trial in resectable locally advanced HNSCC, demonstrated that neoadjuvant plus adjuvant pembrolizumab added to standard therapy significantly improved event-free survival without compromising surgical feasibility 53.
In laryngeal and hypopharyngeal cancer, specifically, induction toripalimab combined with chemotherapy yielded encouraging activity, promising larynx-preservation rates, and acceptable toxicity in a single-arm phase II study 54.
Taken together, these data suggest that immunotherapy is reshaping the treatment landscape in recurrent/metastatic and high-risk resected HNSCC, whereas its optimal role in definitive larynx-preservation regimens remains to be defined.
Proton therapy
Alongside increasingly sophisticated systemic strategies, attention has turned to highly conformal RT techniques. Intensity-modulated proton therapy (IMPT) allows improved dose distributions compared with photon RT, with steep dose fall-off and better sparing of organs at risk. In early-stage glottic cancer, IMPT and modern image-guided techniques have yielded excellent local control with minimal toxicity and high laryngeal function preservation 55. Dosimetric comparisons show that proton techniques can reduce dose to carotid arteries, arytenoid cartilage, pharyngo-laryngeal musculature, thyroid gland, spinal cord and, with image-guided IMRT, the contralateral vocal cord 56-58.
A major challenge of IMPT, particularly in glottic tumours, is its sensitivity to anatomic and density changes during treatment, requiring robust planning and image guidance to avoid marginal misses and motion interplay effects 59.
Early clinical series suggest that proton therapy for laryngeal SCC achieves high OS, locoregional control, and DFS with a favourable toxicity profile 60.
Supportive care and functional outcomes
HNSCC is the seventh most common cancer worldwide, with approximately 700,000 new cases and 350,000 deaths annually 61.
Despite technical and therapeutic advances, survival for laryngeal cancer has remained relatively stable, underlining the importance of supportive care and survivorship.
Treatment selection must integrate tumour factors (site, T/N category, histology), and patient factors (age, comorbidities, baseline function, occupation, preferences). Comprehensive assessment should include nutritional status, cardiopulmonary and renal function, frailty (in older patients), psychosocial context, and dental status, with early nutritional support when weight loss exceeds 10% in 6 months. Multidisciplinary management in high-volume centres is associated with better outcomes 21.
Pretreatment laryngeal function is the strongest predictor of functional rehabilitation after larynx-preserving treatment. Attempts to preserve the larynx in patients with severe pretreatment dysfunction often result in chronic tracheostomy or gastrostomy dependence and are not considered true functional successes.
Late toxicities after RT/CRT include xerostomia, osteoradionecrosis, hypothyroidism, pharyngo-oesophageal stenosis, lymphoedema, and dizziness 62.
Dysphagia is a major issue: up to half of survivors of advanced HNSCC experience clinically significant swallowing impairment, and aspiration is common and frequently under-recognised 63-66.
Dose-volume relationships for swallowing-related structures (pharyngeal constrictors, supraglottic and glottic larynx, submandibular glands) are now well established and have informed “dysphagia-optimised” IMRT planning 67-70.
Speech and swallowing rehabilitation, smoking and alcohol cessation support, psychosocial care, and long-term endocrinologic monitoring (e.g. for hypothyroidism) are integral components of modern laryngeal cancer management. Regular follow-up, including endoscopic examination and neck palpation for at least 5 years, is recommended to detect recurrences early and to manage late toxicities proactively.
Conclusions
Laryngeal SCC remains a complex disease that requires meticulous multidisciplinary evaluation and personalised treatment planning. While early-stage tumours can often be managed effectively with single-modality therapy, advanced-stage disease demands careful selection between organ-preservation strategies and primary surgery to balance oncologic outcomes with functional preservation. CRT remains the cornerstone of nonsurgical management, although survival advantages over surgery are not demonstrated, and functional outcomes vary widely depending on baseline laryngeal function. Attempts to improve outcomes using induction chemotherapy, targeted agents, or immunotherapy have yielded mixed results, with meaningful benefits emerging primarily from rigorously selected neoadjuvant immunotherapy approaches. Advances in RT techniques offer opportunities to reduce toxicity while maintaining disease control. Ultimately, optimal outcomes depend on precise staging, assessment of functional reserve, thoughtful integration of multimodality treatment, and delivery of care within high-volume, experienced centres, ensuring an approach that maximises cure while preserving quality of life whenever possible.
Acknowledgements
Figures were original and created with BioRender.com.
Conflict of interest statement
SC discloses occasional fees for participation as a speaker at conferences/congresses from AccMed; support for attending meetings and/or travel from AccMed, MultiMed Engineers srl, and Care Insight sas, unrelated to the content of this work. LL discloses the following conflicts of interest: research funds donated directly to the institute for clinical trials from AstraZeneca, BMS, Boehringer Ingelheim, Celgene International, Eisai, Exelixis, Debiopharm International SA, Hoffmann-La Roche Ltd, IRX Therapeutics, Medpace, Merck-Serono, MSD, Novartis, Pfizer, Roche, and Buran; occasional fees for participation as a speaker at conferences/congresses or as a scientific consultant for advisory boards from AstraZeneca, Bayer, MSD, Merck-Serono, AccMed, Neutron Therapeutics, Inc., and Alentis. CB declares no conflicts of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
CB, SC: prepared the first draft of the manuscript; LL: supervised, revised the text, and approved the final version.
Ethical consideration
Not applicable.
History
Received: February 3, 2026
Accepted: March 16, 2026
Figures and tables
Figure 1. Challenges in the treatment of laryngeal cancer: the patient at the centre of care.
Figure 2. Treatment algorithm for non-metastatic laryngeal cancer according to ESMO-ESTRO guidelines.
| Ranking | Patients | Companions | Multidisciplinary team |
|---|---|---|---|
| 1 | Being cured of my cancer | Being cured of my cancer | Being cured of my cancer |
| 2 | Living as long as possible | Living as long as possible | Living as long as possible |
| 3 | Having no pain | Having no pain | Having no pain |
| 4 | Able to swallow all foods | Able to swallow all foods | Able to swallow all foods |
| 5 | Having normal energy for me | Having normal energy for me | Keeping my appearance |
| 6 | Returning to my activities | Returning to my activities | Returning to my activities |
| 7 | Speech understood easily | A comfortably moist mouth | Speech understood easily |
| 8 | Keeping natural voice | Speech understood easily | Able to chew normally |
| 9 | A comfortably moist mouth | Able to chew normally | Keeping natural voice |
| 10 | Keeping my appearance | Keeping natural voice | Having normal energy for me |
| 11 | Able to chew normally | Keeping my appearance | A comfortably moist mouth |
| 12 | Normal taste and smell | Normal taste and smell | Normal taste and smell |
References
- Machiels J, Leemans C, Golusinski W. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31:1462-1475. doi:https://doi.org/10.1016/j.annonc.2020.07.011
- Gatta G, Capocaccia R, Botta L. Burden and centralised treatment in Europe of rare tumours: results of RARECAREnet – A population-based study. Lancet Oncol. 2017;18:1022-1039. doi:https://doi.org/10.1016/S1470-2045(17)30445-X
- Parkin D, Bray F, Ferlay J. Global Cancer Statistics, 2002. CA Cancer J Clin. 2005;55:74-108. doi:https://doi.org/10.3322/canjclin.55.2.74
- Hoffman H, Porter K, Karnell L. Laryngeal cancer in the United States: changes in demographics, patterns of care, and survival. Laryngoscope. 2006;116:1-13. doi:https://doi.org/10.1097/01.mlg.0000236095.97947.26
- Ferlito A. The natural history of early vocal cord cancer. Acta Otolaryngol. 1995;115:345-347. doi:https://doi.org/10.3109/00016489509139326
- Marioni G, Marchese-Ragona R, Cartei G. Current opinion in diagnosis and treatment of laryngeal carcinoma. Cancer Treat Rev. 2006;32:504-515. doi:https://doi.org/10.1016/j.ctrv.2006.07.002
- Haapaniemi A, Koivunen P, Saarilahti K. Laryngeal cancer in Finland: a 5-year follow-up study of 366 patients. Head Neck. 2016;38:36-43. doi:https://doi.org/10.1002/hed.23834
- Huang B, Solle M, Weissler M. Larynx: anatomic imaging for diagnosis and management. Otolaryngol Clin North Am. 2012;45:1325-1361. doi:https://doi.org/10.1016/J.OTC.2012.08.006
- Hans S, Baudouin R, Circiu M. Open partial laryngectomies: history of laryngeal cancer surgery. J Clin Med. 2022;11. doi:https://doi.org/10.3390/jcm11185352
- Obid R, Redlich M, Tomeh C. The treatment of laryngeal cancer. Oral Maxillofac Surg Clin North Am. 2019;31:1-11. doi:https://doi.org/10.1016/j.coms.2018.09.001
- Forastiere A, Zhang Q, Weber R. Long-term results of RTOG 91-11: a comparison of three nonsurgical treatment strategies to preserve the larynx in patients with locally advanced larynx cancer. J Clin Oncol. 2013;31:845-852. doi:https://doi.org/10.1200/JCO.2012.43.6097
- Abdurehim Y, Hua Z, Yasin Y. Transoral laser surgery versus radiotherapy: systematic review and meta-analysis for treatment options of T1a glottic cancer. Head Neck. 2012;34:23-33. doi:https://doi.org/10.1002/hed.21686
- Feng Y, Wang B, Wen S. Laser surgery versus radiotherapy for T1-T2N0 glottic cancer: a meta-analysis. ORL J Otorhinolaryngol Relat Spec. 2011;73:336-342. doi:https://doi.org/10.1159/000327097
- Yoo J, Lacchetti C, Hammond J. Role of endolaryngeal surgery (with or without laser) versus radiotherapy in the management of early (T1) glottic cancer: a systematic review. Head Neck. 2014;36:1807-1819. doi:https://doi.org/10.1002/hed.23504
- Mucha-Małecka A, Składowski K. High-dose radiotherapy alone for patients with T4-stage laryngeal cancer. Strahlentherapie Und Onkologie. 2013;189:632-638. doi:https://doi.org/10.1007/S00066-013-0396-0
- Mendenhall W, Dagan R, Bryant C. Definitive radiotherapy for squamous cell carcinoma of the glottic larynx. Cancer Control. 2016;23:208-212. doi:https://doi.org/10.1177/107327481602300303
- Forastiere A, Ismaila N, Lewin J. Use of larynx-preservation strategies in the treatment of laryngeal cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2018;36:1143-1169. doi:https://doi.org/10.1200/JCO.2017.75.7385
- Pignon J, Bourhis J, Domenge C. Chemotherapy added to locoregional treatment for head and neck squamous-cell carcinoma: three meta-analyses of updated individual data. MACH-NC Collaborative Group. Meta-analysis of chemotherapy on head and neck cancer. Lancet. 2000;355:949-955.
- Pignon J-P, le Maître A, Maillard E. MACH-NC Collaborative Group. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 93 randomised trials and 17,346 patients. Radiother Oncol. 2009;92:4-14. doi:https://doi.org/10.1016/j.radonc.2009.04.014
- Lacas B, Carmel A, Landais C. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 107 randomized trials and 19,805 patients, on behalf of MACH-NC Group. Radiother Oncol. 2021;156:281-293. doi:https://doi.org/10.1016/j.radonc.2021.01.013
- Sherman E, Fisher S, Kraus D. TALK score: development and validation of a prognostic model for predicting larynx preservation outcome. Laryngoscope. 2012;122:1043-1050. doi:https://doi.org/10.1002/lary.23220
- Greulich M, Parker N, Lee P. Voice outcomes following radiation versus laser microsurgery for T1 glottic carcinoma. Otolaryngol Head Neck Surg. 2015;152:811-819. doi:https://doi.org/10.1177/0194599815577103
- Chen A, Halpern M. Factors predictive of survival in advanced laryngeal cancer. Arch Otolaryngol Head Neck Surg. 2007;133:1270-1276. doi:https://doi.org/10.1001/archotol.133.12.1270
- Lefebvre J, Rolland F, Tesselaar M. Phase 3 randomized trial on larynx preservation comparing sequential vs alternating chemotherapy and radiotherapy. J Natl Cancer Inst. 2009;101:142-152. doi:https://doi.org/10.1093/jnci/DJN460
- Lefebvre J, Andry G, Chevalier D. Laryngeal preservation with induction chemotherapy for hypopharyngeal squamous cell carcinoma: 10-year results of EORTC trial 24891. Ann Oncol. 2012;23:2708-2714. doi:https://doi.org/10.1093/annonc/mds065
- Henriques De Figueiredo B, Fortpied C, Menis J. Long-term update of the 24954 EORTC phase III trial on larynx preservation. Eur J Cancer. 2016;65:109-112. doi:https://doi.org/10.1016/j.ejca.2016.06.024
- Janoray G, Pointreau Y, Garaud P. Long-term results of a multicenter randomized phase III trial of induction chemotherapy with cisplatin, 5-fluorouracil, ± docetaxel for larynx preservation. J Natl Cancer Inst. 2016;108. doi:https://doi.org/10.1093/jnci/DJV368
- Pointreau Y, Garaud P, Chapet S. Randomized trial of induction chemotherapy with cisplatin and 5-fluorouracil with or without docetaxel for larynx preservation. J Natl Cancer Inst. 2009;101:498-506. doi:https://doi.org/10.1093/jnci/DJP007
- Posner M, Hershock D, Blajman C. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N Engl J Med. 2007;357:1705-1715. doi:https://doi.org/10.1056/NEJMoa070956
- Vermorken J, Remenar E, van Herpen C. Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. N Engl J Med. 2007;357:1695-1704. doi:https://doi.org/10.1056/NEJMoa071028
- Forastiere A, Goepfert H, Maor M. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. 2003;349:2091-2098. doi:https://doi.org/10.1056/NEJMoa031317
- Bonner J, Harari P, Giralt J. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med. 2006;354:567-578. doi:https://doi.org/10.1056/NEJMoa053422
- Bonner J, Giralt J, Harari P. Cetuximab and radiotherapy in laryngeal preservation for cancers of the larynx and hypopharynx: a secondary analysis of a randomized clinical trial. JAMA Otolaryngol Head Neck Surg. 2016;142:842-849. doi:https://doi.org/10.1001/jamaoto.2016.1228
- Batsakis J. Surgical excision margins: a pathologist’s perspective. Adv Anat Pathol. 1999;6:140-148. doi:https://doi.org/10.1097/00125480-199905000-00002
- Bernier J, Domenge C, Ozsahin M. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med. 2004;350:1945-1952. doi:https://doi.org/10.1056/NEJMoa032641
- Cooper J, Pajak T, Forastiere A. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med. 2004;350:1937-1944. doi:https://doi.org/10.1056/NEJMoa032646
- Bernier J, Cooper J, Pajak T. Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck. 2005;27:843-850. doi:https://doi.org/10.1002/hed.20279
- Pardoll D. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12:252-264. doi:https://doi.org/10.1038/nrc3239
- Harrington K, Burtness B, Greil R. Pembrolizumab with or without chemotherapy in recurrent or metastatic head and neck squamous cell carcinoma: updated results of the phase III KEYNOTE-048 study. J Clin Oncol. 2023;41:790-802. doi:https://doi.org/10.1200/JCO.21.02508
- Ferris R, Blumenschein G, Fayette J. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med. 2016;375:1856-1867. doi:https://doi.org/10.1056/NEJMoa1602252
- Chen D, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity. 2013;39:1-10. doi:https://doi.org/10.1016/j.immuni.2013.07.012
- Weichselbaum R, Liang H, Deng L. Radiotherapy and immunotherapy: a beneficial liaison?. Nat Rev Clin Oncol. 2017;14:365-379. doi:https://doi.org/10.1038/nrclinonc.2016.211
- Huguet F, Durand B, Atallah S. Combination of radiation therapy-immunotherapy for head and neck cancers: promises kept?. Cancer Radiother. 2021;25:811-815. doi:https://doi.org/10.1016/j.canrad.2021.08.018
- Schreiber R, Old L, Smyth M. Cancer immunoediting: integrating immunity’s roles in cancer suppression and promotion. Science. 2011;331:1565-1570. doi:https://doi.org/10.1126/science.1203486
- Tao Y, Aupérin A, Sun X. Avelumab-cetuximab-radiotherapy versus standards of care in locally advanced squamous-cell carcinoma of the head and neck: the safety phase of a randomised phase III trial GORTEC 2017-01 (REACH). Eur J Cancer. 2020;141:21-29. doi:https://doi.org/10.1016/j.ejca.2020.09.008
- Powell S, Gold K, Gitau M. Safety and efficacy of pembrolizumab with chemoradiotherapy in locally advanced head and neck squamous cell carcinoma: a phase IB study. J Clin Oncol. 2020;38:2427-2437. doi:https://doi.org/10.1200/JCO.19.03156
- Lee N, Ferris R, Psyrri A. Avelumab plus standard-of-care chemoradiotherapy versus chemoradiotherapy alone in patients with locally advanced squamous cell carcinoma of the head and neck: a randomised, double-blind, placebo-controlled, multicentre, phase 3 trial. Lancet Oncol. 2021;22:450-462. doi:https://doi.org/10.1016/S1470-2045(20)30737-3
- Machiels J, Tao Y, Licitra L. Pembrolizumab plus concurrent chemoradiotherapy versus placebo plus concurrent chemoradiotherapy in patients with locally advanced squamous cell carcinoma of the head and neck (KEYNOTE-412): a randomised, double-blind, phase 3 trial. Lancet Oncol. 2024;25:572-587. doi:https://doi.org/10.1016/S1470-2045(24)00100-1
- Haddad R, Fayette J, Teixeira M. Atezolizumab in high-risk locally advanced squamous cell carcinoma of the head and neck: a randomized clinical trial. JAMA. 2025;333:1599-1607. doi:https://doi.org/10.1001/jama.2025.1483
- Bourhis J, Auperin A, Borel C. NIVOPOSTOP (GORTEC 2018-01): a phase III randomized trial of adjuvant nivolumab added to radio-chemotherapy in patients with resected head and neck squamous cell carcinoma at high risk of relapse. J Clin Oncol. 2025;43. doi:https://doi.org/10.1200/JCO.2025.43.17
- Hecht M, Eckstein M, Rutzner S. Induction chemoimmunotherapy followed by CD8+ immune cell-based patient selection for chemotherapy-free radioimmunotherapy in locally advanced head and neck cancer. J Immunother Cancer. 2022;10. doi:https://doi.org/10.1136/jict-2021-003747
- Uppaluri R, Campbell K, Egloff A. Neoadjuvant and adjuvant pembrolizumab in resectable locally advanced, Human Papillomavirus-unrelated head and neck cancer: a multicenter, phase II trial. Clin Cancer Res. 2020;26:5140-5152. doi:https://doi.org/10.1158/1078-0432.CCR-20-1695
- Uppaluri R, Haddad R, Tao Y. Neoadjuvant and adjuvant pembrolizumab in locally advanced head and neck cancer. N Engl J Med. 2025;393:37-50. doi:https://doi.org/10.1056/NEJMoa2415434
- Ou X, Zhai R, Wei W. Induction toripalimab and chemotherapy for organ preservation in locally advanced laryngeal and hypopharyngeal cancer: a single-arm phase II clinical trial. Clin Cancer Res. 2024;30:344-355. doi:https://doi.org/10.1158/1078-0432.CCR-23-2398
- Held T, Franke H, Lang K. Intensity modulated proton therapy for early-stage glottic cancer: high-precision approach to laryngeal function preservation with exceptional treatment tolerability. Radiat Oncol. 2022;17. doi:https://doi.org/10.1186/s13014-022-02144-w
- Osman S, Astreinidou E, De Boer H. IMRT for image-guided single vocal cord irradiation. Int J Radiat Oncol Biol Phys. 2012;82:989-897. doi:https://doi.org/10.1016/j.ijrobp.2010.12.022
- Matthiesen C, Herman T, Singh H. Dosimetric and radiobiologic comparison of 3D conformal, IMRT, VMAT and proton therapy for the treatment of early-stage glottic cancer. J Med Imaging Radiat Oncol. 2015;59:221-228. doi:https://doi.org/10.1111/1754-9485.12227
- Kato T, Fuwa N, Murakami M. Dose-volume comparison of IMRT and PSPT treatment plans for early-stage glottic cancer. Int J Part Ther. 2020;7. doi:https://doi.org/10.14338/IJPT-20-00008.1
- Maury A, Bosset M, Coutte A. Radiotherapy for laryngeal cancers: 2025 update. Cancer Radiother. 2025;29. doi:https://doi.org/10.1016/j.canrad.2025.104727
- Ausat N, Rosenthal D, Gunn G. Outcomes following proton therapy for squamous cell carcinoma of the larynx. Int J Radiat Oncol Biol Phys. 2020;106. doi:https://doi.org/10.1016/j.ijrobp.2019.11.081
- Bray F, Ferlay J, Soerjomataram I. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394-424. doi:https://doi.org/10.3322/caac.21492
- Brook I. Late side effects of radiation treatment for head and neck cancer. Radiat Oncol J. 2020;38:84-92. doi:https://doi.org/10.3857/roj.2020.00213
- Eisbruch A, Lyden T, Bradford C. Objective assessment of swallowing dysfunction and aspiration after radiation concurrent with chemotherapy for head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2002;53:23-28. doi:https://doi.org/10.1016/S0360-3016(02)02712-8
- Hutcheson K, Barringer D, Rosenthal D. Swallowing outcomes after radiotherapy for laryngeal carcinoma. Arch Otolaryngol Head Neck Surg. 2008;134:178-183. doi:https://doi.org/10.1001/archoto.2007.33
- Nguyen N, Frank C, Moltz C. Aspiration rate following chemoradiation for head and neck cancer: an underreported occurrence. Radiother Oncol. 2006;80:302-306. doi:https://doi.org/10.1016/j.radonc.2006.07.031
- Nguyen N, Sallah S, Karlsson U. Combined chemotherapy and radiation therapy for head and neck malignancies: quality of life issues. Cancer. 2002;94:1131-1141. doi:https://doi.org/10.1002/cncr.10257
- Eisbruch A, Kim H, Feng F. Chemo-IMRT of oropharyngeal cancer aiming to reduce dysphagia: swallowing organs late complication probabilities and dosimetric correlates. Int J Radiat Oncol Biol Phys. 2011;81:E93-E99. doi:https://doi.org/10.1016/j.ijrobp.2010.12.067
- Söderström K, Nilsson P, Laurell G. Dysphagia – Results from multivariable predictive modelling on aspiration from a subset of the ARTSCAN trial. Radiother Oncol. 2017;122:192-199. doi:https://doi.org/10.1016/j.radonc.2016.09.001
- Petkar I, Bhide S, Newbold K. Dysphagia-optimised intensity-modulated radiotherapy techniques in pharyngeal cancers: is anyone going to swallow it?. Clin Oncol. 2017;29:E110-E118. doi:https://doi.org/10.1016/j.clon.2017.02.002
- Ward M, Adelstein D, Bhateja P. Severe late dysphagia and cause of death after concurrent chemoradiation for larynx cancer in patients eligible for RTOG 91-11. Oral Oncol. 2016;57:21-26. doi:https://doi.org/10.1016/j.oraloncology.2016.03.014
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 648 times
- PDF downloaded - 162 times