Annual congress report
Vol. 46: 112 TH CONGRESS SIOECHCF - OFFICIAL REPORT 2026
The histopathological spectrum of laryngeal epithelial neoplasia
Summary
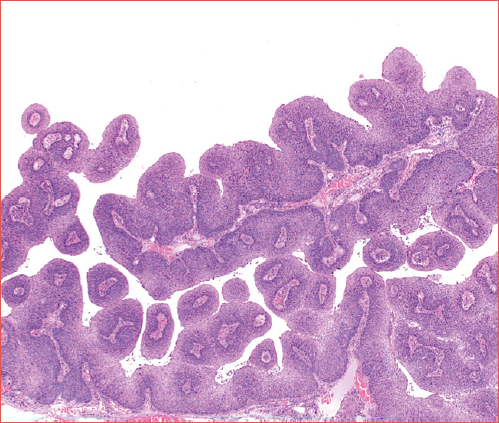
Cover Image
The larynx may harbour a wide spectrum of benign, precursor, and malignant lesions. While benign entities predominate, malignant tumours – most commonly keratinising squamous cell carcinoma – pose significant diagnostic and therapeutic challenges due to their histologic and biological heterogeneity. Accurate histopathological evaluation is therefore essential for appropriate classification, prognostication, and optimal clinical management of laryngeal neoplasms. This review outlines the principal pathological features of laryngeal precursor lesions and malignant neoplasms, with emphasis on conventional squamous cell carcinoma and its major variants. Key differential diagnostic considerations and prognostic implications are discussed, along with a brief overview of emerging biomarkers and immunotherapeutic strategies for advanced and recurrent disease.
Introduction
The larynx, essential for respiration and phonation, has a complex anatomy with multiple tissue types working in unison to perform its functions. This structural complexity makes it susceptible to a variety of pathologies, including neoplastic lesions, which are both common and heterogeneous in type ranging from benign, pre-malignant to malignant with metastatic potential.
Benign lesions are the most common laryngeal pathologies, outnumbering malignant lesions. They include squamous papillomas, haemangiomas, laryngeal nodules, cysts, polyps, and Reinke’s oedema. These lesions are often associated with voice abuse, chronic irritation, smoking, or viral infections (e.g., human papilloma virus [HPV] for papillomas) and typically present with hoarseness, dysphonia, or airway symptoms depending on size and location. Even though benign, some lesions – particularly papillomas – may recur and, rarely, undergo malignant transformation.
Although benign lesions predominate, malignant neoplasms of the larynx can arise and present significant clinical challenges. Laryngeal cancers are relatively rare, representing approximately 3% and 0.6% of all newly diagnosed malignancies in Italy and United States, respectively 1. Their prevalence is higher in Asia and Europe compared with Northern and Latin America, Africa, and Oceania.
Among malignancies of the hypopharynx, larynx, and trachea, 90-98% originate from the overlying epithelium, and about 90% of these are conventional keratinising squamous cell carcinomas (SCC) 2,3. Histologic variants – including verrucous, papillary, spindle cell, basaloid, adenosquamous, and lymphoepithelial types – make up less than 10% of cases 4,5. Each variant exhibits distinct morphological, molecular, and prognostic features and can mimic other tumour types, emphasising the importance of accurate histopathological diagnosis. Tobacco smoking is the principal risk factor for nearly all laryngeal SCCs, with alcohol contributing modestly in non-smokers, while high-risk HPV infection is rare, reported in only ~2% of cases in Italian series 6,7.
Although SCC is the predominant malignant laryngeal tumour, a minority of cases are represented by less common epithelial, mesenchymal, and haematolymphoid neoplasms. These include neuroendocrine carcinomas, minor salivary gland tumours – such as adenoid cystic, mucoepidermoid, and myoepithelial carcinomas, more often located in the trachea – and mesenchymal malignancies, most commonly low-grade chondrosarcoma of the cricoid or thyroid cartilage. Rarer entities include embryonal or alveolar rhabdomyosarcoma, inflammatory myofibroblastic tumour, synovial sarcoma, and well- or dedifferentiated liposarcoma 8. Haematolymphoid neoplasms, including extramedullary plasmacytoma and mucosa-associated lymphoid tissue (MALT) lymphoma, preferentially involve the supraglottic and subglottic regions 9.
Precursor lesions, commonly referred to as dysplasia or squamous intraepithelial lesions, represent a continuum of histopathological alterations with potential for malignant transformation. They are graded as mild, moderate, or severe dysplasia based on the degree of cellular atypia and architectural disarray. However, the classification and clinical management of these lesions remain subjects of ongoing debate, reflecting the complexity of predicting progression to invasive carcinoma.
Overall, the spectrum of benign, precursor, and malignant laryngeal lesions reflects the diverse pathological landscape of the larynx and emphasises the clinical importance of accurate histopathological evaluation of both common and rare neoplasms, including unusual subtypes, alongside timely and appropriate management tailored to the specific pathology.
Precursor lesions
Papillomas and papillomatosis
Laryngeal squamous papilloma (LSP) is the most common benign epithelial tumour of the larynx, typically arising at squamous-ciliated epithelial junctions, most often involving the true vocal cords and laryngeal ventricles, with possible extension to adjacent subsites and, rarely, the lower respiratory tract, where involvement is associated with high mortality 10-12. LSP shows a bimodal age distribution, with a juvenile form presenting around 2-3 years of age that is frequently multifocal along the respiratory tract and recurrent (recurrent respiratory papillomatosis), and an adult form occurring in early adulthood (20-40 years) that is usually solitary 13,14. Over 90% of cases are associated with low-risk HPV types 6 and 11, where coinfection with additional low- or rarely high-risk HPV types may occur 15-17. Juvenile disease is most often attributed to vertical transmission at birth, with increased risk associated with young maternal age, vaginal delivery, and first-born status.
Histologically, LSPs are small exophytic epithelial tumours composed of papillary fronds with central fibrovascular cores (Fig. 1A). The overlying hyperplastic squamous epithelium typically shows minimal surface keratinisation, and koilocytic change in the superficial layers is not infrequent (Fig. 1B). Foci of epithelial dysplasia and malignant transformation are uncommon but have been reported, occurring in approximately 21 and 4% of cases, respectively, particularly in the context of smoking, prior irradiation, or long-standing disease 13,18-21.
The clinical course is unpredictable, ranging from spontaneous remission to aggressive, recurrent disease requiring repeated surgical intervention. Although a consistent correlation between HPV genotype and clinical aggressiveness has not been established, accumulating evidence supports a beneficial role for prophylactic and therapeutic bivalent and tetravalent HPV vaccination in reducing disease incidence and severity, irrespective of HPV strain 14,22,23.
Dysplasia
Laryngeal epithelial dysplasia represents premalignant epithelial changes driven by accumulated genetic alterations, most commonly affecting the true vocal cords, with rare involvement of commissures, hypopharynx, or trachea 24-26. Clinical presentation is non-specific and site-dependent, with hoarseness typical of glottic lesions 27.
Epithelial dysplasia predominantly affects older males (male to female ratio up to 5:1), with cigarette smoking – often combined with alcohol – being the principal risk factor; gastro-oesophageal reflux and HPV play minor roles 28-35.
Histologically, dysplasia shows cytologic and architectural atypia, with or without keratinisation. The epithelium is usually thickened but may appear normal or atrophic. Preservation of the basement membrane and absence of desmoplastic stroma are key features. Grading remains essential for prognosis, with 2- and 3-tiered systems based on epithelial thickness involvement by cellular atypia – less than lower half, beyond lower half, or full thickness – classifying lesions as low- (Fig. 2A), high-grade (Fig. 2B), or carcinoma in situ (Fig. 2C) 36. These tiers may also be grouped into low- (L-SIL) and high-grade squamous intraepithelial lesion (H-SIL), similar to oral and lower genital tract lesions 37-41.
Malignant progression of laryngeal epithelial dysplasia correlates with grade, with transformation rates of approximately 1.6% for low-grade and 12.5% for high-grade lesions. Carcinoma in situ may progress in up to 40% of cases, particularly in patients with tobacco or alcohol exposure or involvement of the anterior commissure 42,43. While laryngeal dysplasia has no formal staging, carcinoma in situ is classified as Tis according to the UICC/AJCC TNM system.
Laryngeal carcinomas
Conventional keratinising squamous cell carcinoma
Laryngeal keratinising squamous cell carcinoma (LKSCC) is called thus to highlight its typically abundant keratinisation and to distinguish it from other histologic subtypes of SCC. It is the second most common respiratory tract cancer and accounts for 25% of head and neck cancers 44,45. More recent data suggest a world-wide decrease in annual age-standardised incidence rate of laryngeal cancer from 1990 to 2017 46.
LKSCC most commonly involves the glottis (60-75%) and supraglottis (25-40%), while subglottic disease is rare (< 5%) 47-50. Clinical presentation varies by tumour location: hoarseness is typical of glottic and supraglottic tumours, whereas larger lesions may lead to dysphagia, odynophagia, or airway compromise. LKSCC predominantly affects men, with a peak incidence between the fifth and seventh decades, and occurs more frequently in European and Northern American populations 3,51.
Tobacco smoking and high-volume alcohol consumption are the principal risk factors, acting synergistically in a dose-dependent manner, with a substantial reduction in risk following prolonged smoking cessation 6,52. Gastro-oesophageal reflux, opium use, and immunodeficiency may also contribute to disease risk, whereas high-risk HPV appears to play only a marginal role 53-56. Exceptionally rare cases have been reported in the paediatric population, in which HPV infection and syndromic conditions involving DNA repair defects or immunosuppression appear to be more prevalent 57-59.
Grossly, LKSCC typically appear as firm, white lesions that are often ulcerated and may exhibit exophytic, endophytic, or mixed growth patterns. Supraglottic tumours can extend into the pre-epiglottic space, while glottic lesions may cross the lateral ventricles. Histologically, neoplastic cells form irregular nests with stromal invasion and a desmoplastic reaction. Tumours are graded according to differentiation, nuclear features, mitotic activity, and keratinisation using a 3-tiered system. Well-differentiated tumours closely mimic stratified epithelium, with maturing cells arranged in layered patterns and showing irregular keratinisation, most typically forming keratin pearls (Fig. 3A). In contrast, moderately and poorly differentiated tumours consist of more immature cells exhibiting nuclear pleomorphism and atypical mitotic figures, with little to no evidence of organised stratification or keratin production (Fig. 3B-C). Immunohistochemically, tumours express a wide array of cytokeratins and p63/p40. Markers such as NUT, CEA, neuroendocrine markers, and TTF1 are typically negative, aiding in differential diagnosis.
From a genetic standpoint, LKSCC may harbour TP53 mutations in approximately 50% of cases 60. However, these mutations are not specific to this entity, as they are commonly observed in epithelial neoplasms, including squamous dysplasia and less common laryngeal histotypes such as lymphoepithelial carcinoma of the larynx 61. Additional molecular alterations that have been described include CDKN2A inactivation, PIK3CA mutations, and, rarely, microsatellite instability.
LKSCC is often characterised by spread to regional lymph nodes (40% of cases and more frequent in supraglottic sites due to their richer lymphatic drainage) and, less commonly, to distant sites (10% of cases) such as the lungs, liver, and bone 62. Occult cervical metastases occur in approximately 20% of clinically node-negative cases, and extranodal extension is associated with poor prognosis. Five-year survival is site-dependent: glottic 75-80%, supraglottic 45-50%, subglottic lower, with an overall average of ~65% 63,64. While histological grade has shown controversial results, prognosis is chiefly determined by tumour stage, nodal status, and both microscopic and macroscopic extranodal extension 65,66. Additional influence on patient prognosis is determined by anterior commissure involvement, tumour budding, perineural invasion, and submucosal spread 67-72. The location of LKSCC affects patient prognosis, with subglottic and supraglottic tumours generally demonstrating poorer survival compared with glottic SCCs, due to delayed presentation and increased likelihood of recurrence and lymph node metastasis 48,50. Surgical margins are critical in advanced disease, whereas early-stage glottic tumours tolerate narrower margins 73,74. Survival is also affected by gender (improved survival in females), age (improved survival in patients < 40 years), and comorbidities 75-77.
Treatment of choice for LKSCC may depend on stage, localisation, tumour extension, and patient choice. Early-stage glottic lesions may undergo simple cordectomy, whereas advanced disease may warrant total laryngectomy with bilateral lymph node dissection and adjuvant (chemo-)radiotherapy. Anti-PD-L1 immunotherapy in patients showing positive PD-L1 status (CPS ≥ 1 or ≥ 20) has shown improved outcomes in recurrent or metastatic cases 78,79.
Basaloid squamous cell carcinoma
Laryngeal basaloid squamous cell carcinoma (LBSCC) derives its name from the characteristic “blue cell”/basaloid histologic appearance and was first described by Wain et al. in 1986 in a series of 10 cases 80. LBSCC is the variant most likely to be mistaken for other tumours, particularly those arising from minor salivary glands. Unlike conventional LKSCC, the vast majority of LBSCCs are supraglottic or involve the piriform sinus. Beyond anatomic location, however, LBSCC is clinically indistinguishable from typical laryngeal SCC and shows essentially the same demographic profile, most commonly affecting adult or elderly Caucasian men.
Despite its morphology, which might suggest a strong HPV association, LBSCC generally does not harbour detectable HPV and typically lacks p16 overexpression, even though earlier studies demonstrated HPV by polymerase chain reaction in basaloid SCCs from other head and neck subsites 81,82.
Grossly, lesions present as a nonspecific tan-white, firm, often ulcerated masses. Histologically, LBSCC is characterised by a proliferation of malignant, primitive-appearing epithelial cells with scant cytoplasm and a high nuclear-to-cytoplasmic ratio (Fig. 4A). The nuclei are hyperchromatic, usually without prominent nucleoli, and may exhibit nuclear moulding and peripheral palisading. Some tumours show marked nuclear pleomorphism, while others appear more monomorphic. The basaloid cells form solid nests and cords that, at low power, have been described as having a “jigsaw puzzle” pattern. Mitotic activity and apoptosis are abundant. Keratinisation is absent, and “comedo-type” necrosis frequently fills the centres of tumour nests, sometimes with small cystic spaces containing mucin-like material. More than 60% of tumours display a sclero-hyalinised, brightly eosinophilic stroma. Focal areas of squamous differentiation or adjacent keratinising squamous dysplasia/in situ carcinoma are often present.
Immunohistochemically, LBSCC shows strong positivity for pan-cytokeratin (Fig. 4B) and p40 (Fig. 4C). Up to 60% of cases may also exhibit multifocal SOX10 positivity (Fig. 4D), a feature that may complicate distinction from certain salivary gland tumours, particularly solid-type adenoid cystic carcinoma 83. LBSCC is generally negative for synaptophysin, chromogranin, NUT, p16, and HPV by in situ hybridisation. These immunophenotypic features, combined with morphology, aid in differentiating LBSCC from other epithelial malignancies, such as neuroendocrine carcinomas, NUT carcinoma, and metastatic oropharyngeal non-keratinising SCC.
Although the literature contains some conflicting reports regarding the clinical behaviour of basaloid compared to conventional SCC – partly due to inclusion of more indolent HPV-associated basaloid oropharyngeal cases – major studies consistently regard LBSCC as an aggressive subtype of laryngeal SCC 84-86. It is associated with poorer disease-specific survival regardless of stage or tumour site. Furthermore, lymph node metastasis occurs in up to 70% of cases and distant metastasis in 35-40%. This markedly aggressive clinical course, compared with conventional LKSCC and HPV-associated basaloid oropharyngeal SCC, highlights the need for comprehensive evaluation for distant metastases and an appropriately aggressive therapeutic strategy 87,88.
Verrucous carcinoma
Verrucous carcinoma was first recognised under unusual circumstances, giving it a particularly notable history. Although various authors initially have described the entity under different names, the term “verrucous carcinoma” was first coined by Ackerman in 1948, who reported 31 cases of a distinct head and neck SCC. Early in his experience, several biopsies were misdiagnosed as “papilloma” due to the tumour’s deceptively benign histology. The lesion’s locally invasive potential became evident when a patient presented with a large tumour eroding through the cheek. Its warty or exophytic appearance and well-differentiated epithelium often led to misclassification, ultimately resulting in its recognition as verrucous carcinoma.
In 1966, Kraus and Perezmesa were the first to report cases of verrucous carcinoma originating in the larynx 89. Although the larynx is the second most frequent site of verrucous carcinoma – accounting for roughly 10-35% of cases – it represents only 1-2% of all laryngeal SCCs, with recent data suggesting a declining incidence between 2000 and 2010 90,91. Nearly 80% of laryngeal lesions involve the glottis, followed by the supraglottis and subglottis 91,92. Laryngeal verrucous squamous cell carcinoma (LVSCC) primarily affects older adults, with a slightly higher age of onset and a pronounced male predominance (male to female ratio 12-14:1) compared with conventional SCC, and is strongly associated with tobacco use 93. While earlier studies suggested that approximately 45% of LVSCC cases harboured high-risk HPV, more recent evidence indicates that LVSCC is not associated with transcriptionally active HPV, even in tumours showing p16 positivity 94-96.
Clinically, LVSCC typically presents with hoarseness, reflecting its characteristic localisation and often bulky morphology. Macroscopically, the tumour is exophytic and broad-based with pushing margins. Microscopically, using strict diagnostic criteria, LVSCC is composed of well-differentiated, acanthotic and hyperkeratotic squamous epithelium forming broad, undulating, and crowded verrucous-like projections (Fig. 5A). The neoplastic cells have ample eosinophilic cytoplasm while mitotic activity and nuclear atypia is minimal and generally confined to basal or suprabasal layers (Fig. 5B). The tumour grows in a pushing, non-infiltrative pattern with a smooth stromal interface and a dense lymphoplasmacytic infiltrate 92,97. Invasion below the level or neighbouring epithelium occurs through expansion of the existing epithelial tongues, without accompanying stromal desmoplasia, and may be challenging to assess on superficial biopsies. In approximately 10-20% of cases, LVSCC may coexist with areas of conventional invasive LKSCC, further complicating diagnosis and necessitating more aggressive management due to the associated metastatic potential 98.
The differential diagnosis includes verrucous hyperplasia, pseudoepitheliomatous hyperplasia, and invasive well-differentiated LKSCC. Verrucous hyperplasia lacks true invasion beneath the adjacent normal epithelium and is exceedingly rare in the larynx compared with the oral cavity. Pseudoepitheliomatous hyperplasia similarly shows no true invasion and lacks the dense, glassy cytoplasm and bulbous rete ridges characteristic of LVSCC, while typically demonstrating more pronounced inflammation. In contrast, invasive well-differentiated LKSCC is defined by an irregular infiltrative growth pattern, associated stromal desmoplastic reaction, and more pronounced cytologic atypia.
LVSCC demonstrates markedly better outcomes than conventional laryngeal SCC, with reported 5-year survival rates of 85-95% and an extremely low likelihood of nodal involvement (0.6%) or distant metastasis 91,99. Most patients present with Stage I disease, and although the tumour exhibits locally destructive, pushing growth, the main clinical concern is local recurrence – particularly when excision is incomplete 100. Surgical resection remains the preferred treatment modality 101. Radiotherapy may be effective, but its use has been linked to increased complications and, rarely, progression to more aggressive tumour variants 102.
Papillary squamous cell carcinoma
Laryngeal papillary squamous cell carcinoma (LPSCC) is a rare histologic variant, accounting for approximately 0.5% of all laryngeal SCC. It occurs predominantly in men, with a reported male to female ratio of about 3:1, and most commonly arises from the glottic or supraglottic mucosa. Unlike papillomas, from which these tumours seldom originate, LPSCC typically develops de novo, with the exception of rare cases arising after therapeutic irradiation. Owing to their exophytic growth and voluminous nature, patients usually present with symptoms related to mucosal irritation or airway compromise, such as dysphonia, progressive airway obstruction, sore throat, cough, dysphagia, or haemoptysis.
Risk factors mirror those of conventional laryngeal SCC, including tobacco and alcohol exposure. In addition, high-risk HPV infection and p16 overexpression have been identified in up to one-third of LPSCCs (Fig. 6B). This rate is substantially lower than that seen in non-keratinising papillary squamous cell carcinoma of the oropharynx – virtually all cases – and in the sinonasal tract, where HPV is present in roughly 68% 103,104. Overall, HPV-related oncogenesis plays a more limited role in the larynx than in other head and neck subsites.
Macroscopically, LPSCC presents as a soft, friable papillary mass of variable size, typically without obvious keratinisation. Histologically, the defining feature is the presence of numerous complex, branching papillae supported by fibrovascular cores and lined by neoplastic squamous epithelium (Cover figure). Although no universal cut-off exists, most studies diagnose LPSCC when papillary architecture comprises at least 50-70% of the lesion. The epithelium covering the fibrovascular cores is predominantly non-keratinizing and exhibits clear malignant features, including nuclear atypia, a high nuclear-to-cytoplasmic ratio, absent maturation, and mitotic figures extending to the surface (Fig. 6A). Less commonly, tumours show keratinising features such as intracellular keratinisation, dyskeratosis, or high-grade keratinising atypia. Koilocytic change may also be present, although it does not necessarily indicate HPV infection 105,106.
Assessment of stromal invasion may be challenging – particularly in small or superficial biopsies – because the papillary fronds often extend across multiple planes and may comprise most of the sampled tissue. When invasion is present, the infiltrative component typically forms irregular nests and tongues of tumour cells resembling those of non-keratinising SCC, often accompanied by desmoplasia or associated inflammation.
When strict histopathologic criteria are applied, LPSCC demonstrates a more favourable prognosis than either exophytic LKSCC or conventional keratinising SCC, independent of HPV status 106. Most cases are diagnosed at an early stage, typically T1 and Stage I. Up to 84% of patients present without nodal involvement (N0), and distant metastases are exceedingly rare, occurring in approximately 1% of cases. Survival outcomes are excellent, with 5-year survival approaching 100% and disease-specific survival at 1, 5, and 10 years reported as 97.1, 83.1, and 73.9%, respectively – significantly higher than those of other laryngeal malignancies 107.
Spindle cell squamous cell carcinoma
Laryngeal spindle cell squamous cell carcinoma (LScSCC) – also known as spindle cell or sarcomatoid carcinoma – is a rare variant of SCC, representing less than 1% of all laryngeal malignancies 108. Unlike other laryngeal cancers, its incidence has remained relatively stable over recent decades (2000-2011). The oral cavity and pharynx are also common sites of origin 109.
First described by Virchow in 1863 as a carcinosarcoma, the tumour was later redefined by Figi et al. in 1933 as an epithelial neoplasm exhibiting spindle cell differentiation. LScSCC occurs predominantly in middle-aged to elderly men (male to female ratio ≈ 7:1) and shows a strong association with tobacco and alcohol exposure, whereas transcriptionally active HPV infection is rare and not associated with improved prognosis 110. Prior irradiation has also been identified as a significant risk factor, with radiation-associated tumours generally demonstrating poorer outcomes than de novo cases 108 .
Most LScSCCs originate in the glottic (72%) or supraglottic (16%) regions, typically presenting with early symptoms such as hoarseness, leading to Stage I diagnosis in approximately 60% of patients 111,112. Grossly, the tumour appears as a bulky, pedunculated, or sessile mass with an ulcerated, exudative surface.
Microscopically, LScSCC exhibits a superficial squamous component – which may display dysplasia, carcinoma in situ, or invasive features – combined with a deeper spindle cell proliferation, usually arranged in fascicular patterns and showing pleomorphism and increased mitotic activity (Fig. 7A-B). Hypocellular variants with bland cytology have been described. Heterologous differentiation, including osseocartilaginous or rhabdomyoblastic elements, occurs rarely and does not influence prognosis 113,114. On immunohistochemistry, the spindle cell component may range from focally positive to completely negative for pan-cytokeratin cocktails (Fig. 7C) or p40 (Fig. 7D), while typically showing diffuse vimentin positivity. In adult and elderly patients, it is customary to classify malignant spindle cell neoplasms of the larynx as LScSCC, regardless of the degree of epithelial or squamous marker expression.
Local recurrence is common, occurring in up to 50% of cases, while regional metastases and distant spread are reported in approximately 13% and less than 4%, respectively 115. Although metastatic disease appears less frequent than in conventional LKSCC, the 10-year disease-specific survival rate – approximately 58% – is similar to that of conventional LKSCC 112. Surgical resection remains the preferred treatment modality and offers the most favourable outcomes, particularly when combined with radiotherapy. In contrast, the therapeutic benefit of radiotherapy or chemotherapy as standalone treatments remains uncertain.
Adenosquamous carcinoma
Adenosquamous carcinoma is a rare and aggressive biphasic epithelial tumour of the head and neck, with the larynx representing the most commonly affected site and showing comparatively more favourable outcomes 116. Laryngeal adenosquamous carcinoma (LASC) predominantly affects men (male to female ratio 2-19:1), typically in the seventh to eighth decades of life, with no clear racial predilection. The glottis is the most frequent site of origin (47.1%), followed by the supraglottis (42.6%), with the subglottis comprising the remainder 117. Symptoms resemble those of other laryngeal malignancies and commonly include hoarseness, dysphagia, or haemoptysis.
Only small case series have described LASC, indicating cigarette smoking and alcohol consumption as the primary associated risk factors. In contrast, HPV infection has not been implicated at this site.
Grossly, LASC may present as a polypoid mass or as areas of mucosal thickening or ulceration. Microscopically, it demonstrates a biphasic pattern with both squamous and glandular differentiation. The squamous component – typically predominant – is more superficial and often associated with dysplastic surface epithelium (Fig. 8A). Variable keratinisation and basaloid or clear cell features may be present 118. The glandular component resides deeper and forms cribriform, tubulo-glandular, or “punched-out” structures. Mucin production is common but not required for diagnosis 119,120. Although most cases show clear separation between the 2 components, intermixed or transitional patterns may occur (Fig. 8B). Necrosis, frequent mitoses, and vascular or perineural invasion are often observed.
LASC presents several diagnostic challenges, making precise identification crucial due to its significantly more aggressive nature. A primary difficulty is that the glandular component often lies deeper within the tissue and may be absent in superficial biopsy samples, raising the risk of misdiagnosis. Furthermore, distinguishing LASC from similar tumours – such as mucoepidermoid, adenoid cystic, and SCC with pseudo-glandular features – can be problematic. Mucoepidermoid carcinoma typically features a mixture of squamous and glandular cells, is associated with MAML2 gene rearrangements, and lacks surface mucosal dysplasia or keratinisation. Adenoid cystic carcinoma is characterised by a biphasic cellular pattern, diverse growth forms, mucin production, and MYB or MYBL1 gene fusions. In contrast, SCC with pseudo-glandular features usually shows pseudo-glandular architecture predominantly at the surface, while maintaining strong p40 expression.
LASC is a highly aggressive histotype associated with poor long-term outcomes, with 5-year survival rates ranging from 30% to 50% and over 55% of cases presenting at advanced stages 116. Loco-regional lymph nodes metastases occur in up to 39% of patients (18.5% N1; 22.2% N2), affecting either or both tumour components, while approximately 10% develops distant metastases 117.
As with LKSCC, the mainstay of treatment for LASC is surgical resection. Currently, there are no widely accepted indications for adjuvant postoperative radiotherapy or chemotherapy 116,121.
Lymphoepithelial carcinoma
Laryngeal lymphoepithelial carcinoma (LLEC) is an exceedingly rare histologic subtype, accounting for approximately 0.2% of laryngeal neoplasms 122,123. Within the upper aerodigestive tract, this histotype most commonly arises in the larynx, with the supraglottic region – particularly the laryngeal ventricles and epiglottis – involved in up to 2/3 of cases. Primary involvement of the hypopharynx/piriform sinus and the glottis is less frequent, while tracheal cases are rare. LLEC shows a marked predilection for older Caucasian men (mean age, 62 years), mirroring the demographic distribution of conventional laryngeal SCC and contrasting with lymphoepithelial nasopharyngeal carcinoma, which predominantly affects individuals of Asian descent 124.
From a pathogenetic standpoint, the association of LLEC with Epstein-Barr virus (EBV) and HPV remains controversial. EBV positivity has been demonstrated in up to 25% of cases, representing a substantially lower incidence than that observed in lymphoepithelial carcinomas arising from the nasopharyngeal mucosa 61,125-130. In contrast, tobacco use and alcohol consumption appear to represent more consistent etiologic risk factors 131.
Grossly, LLEC typically presents as an ulcerated, raised or depressed mucosal lesion, often causing hoarseness, dysphonia, dysphagia, and occasionally haemoptysis. Histologically, it is composed of sheets (Regaud pattern) or nests (Schmincke pattern) of poorly differentiated malignant epithelioid cells with indistinct cell borders, forming a syncytial growth pattern. The tumour cells are embedded in a dense lymphoplasmacytic stroma and exhibit vesicular nuclei, prominent nucleoli, and frequent mitotic figures, with minimal or absent keratinisation. Rarely a superficial in situ carcinomatous component or associated foci of conventional LKSCC have been described. To date there is no evidence showing a difference in clinical behaviour based on the presence of a LKSCC component. Immunohistochemically, LLEC demonstrates diffuse positivity for multiple cytokeratins (AE1/AE3, MNF116) and p63/p40, confirming epithelial and squamous differentiation. EBV-encoded RNA in situ hybridisation is typically negative in the majority of cases. The immunohistochemical profile of LLEC aids in the distinction from other neoplasms that may be close mimics (e.g. melanoma or lymphoma).
Owing to its rarity and limited clinical data, standardised staging and optimal management strategies for lymphoepithelial carcinoma of the larynx, hypopharynx, and trachea remain undefined. Reported biological behaviour is variable; however, LLEC frequently shows aggressive clinical features with early regional and distant dissemination, including lymph node metastases in 50-75% of cases and distant metastases in approximately 25% 132. Metastatic deposits may retain typical lymphoepithelial morphology or exhibit keratinising squamous differentiation when present in the primary tumour. The reported 5-year disease-specific survival rate is approximately 65-70% 124. Treatment in most series has consisted of surgical resection with neck dissection and adjuvant (chemo-)radiotherapy, although several studies have demonstrated marked radiosensitivity, supporting radiotherapy as a potential organ-preserving approach in early-stage disease 123,130,132-136.
Biomarkers and immunotherapeutic opportunities for advanced and recurrent disease
Treatment paradigms and survival outcomes for conventional LKSCC are well established through large multicentre studies, whereas evidence for rare histologic variants is often limited to small case series. These primary SCC variants differ in histologic and biologic behaviour, making accurate diagnosis essential. Advances in molecular profiling, HPV testing, and biomarker research are likely to enable more tailored therapeutic strategies.
Standard management of advanced laryngeal SCC includes surgery, (chemo-)radiation, or combined modality approaches. Landmark trials have demonstrated the efficacy of induction chemotherapy followed by radiation and concurrent chemoradiotherapy for organ preservation 137-141.
In the setting of non-curable, locally advanced, recurrent, or metastatic head and neck cancer in fit patients, immune checkpoint inhibition (ICI) has emerged as an important therapeutic option. As endorsed by the 2021 AIOM guidelines among others, a combination of anti-PD-1 agents and platinum-based chemotherapy may be considered 79,142. Programmed death-ligand 1 (PD-L1) expression, assessed by the combined positive score (CPS), helps identify patients most likely to benefit from anti-PD-1 ICI agents such as pembrolizumab and nivolumab, which improve survival and induce durable responses 143. Although higher PD-L1 levels (CPS ≥ 20) generally correlate with an immunosuppressive microenvironment and advanced disease, responses have also been observed in PD-L1-low tumours (CPS < 1), highlighting the need for additional predictive biomarkers to optimise patient selection.
However, a small subset of patients treated with ICI may experience an unusually rapid worsening of disease, known as hyperprogression, which correlates with shorter progression-free survival 144. Additionally, numerous ongoing clinical trials are investigating further immunotherapeutic approaches for patients with head and neck squamous cell carcinoma, including promising combinations of ICI with multi-targeted kinase inhibitors and other anti-angiogenic agents 145.
Acknowledgements
The authors would like to thank all researchers whose work contributed to this review.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
All authors of the paper contributed equally to this work.
Ethical consideration
Not applicable.
History
Received: February 6, 2026
Accepted: February 11, 2026
Figures and tables
Figure 1. Histology of a laryngeal papilloma showing finger-like projections of stratified squamous epithelium with fibrovascular cores (A). Mild cytologic atypia and absence of mitotic activity above the basal layer are characteristic (B).
Figure 2. Morphologic spectrum of laryngeal squamous epithelial dysplasia, often associated with submucosal lymphocytic infiltration. Low-grade dysplasia shows mild atypia confined to the basal third with hyperkeratosis (A); higher-grade dysplasia shows moderate to severe atypia involving more than two-thirds of the epithelium (B); carcinoma in situ demonstrates full-thickness severe cytologic and architectural atypia with an intact basement membrane (C).
Figure 3. Histologic spectrum of squamous cell carcinoma differentiation: well-differentiated (A), moderately differentiated (B), and poorly differentiated (C), showing progressive loss of keratinisation, cellular cohesion, and maturation.
Figure 4. Histopathological features of laryngeal basaloid squamous cell carcinoma. The tumour is composed of solid nests and cords of basaloid cells with scant cytoplasm, nuclear hyperchromasia, lacking overt keratinisation (A). Immunostains show diffuse positivity for pan-cytokeratin (MNF116) (B) and p40 (C), confirming squamous differentiation. SOX10 shows multifocal nuclear positivity (D), a rare but previously reported finding in basaloid SCC.
Figure 5. Histological features of laryngeal verrucous squamous cell carcinoma showing broad, undulating, hyperkeratotic projections with acanthotic epithelium and a characteristic pushing tumour border (A). The neoplastic epithelium exhibits minimal atypia and rare basal mitoses, and the non-infiltrative interface demonstrates dense lymphoplasmacytic inflammation without desmoplasia (B).
Figure 6. Laryngeal papillary squamous cell carcinoma. The tumour demonstrates branching papillary architecture and is composed of stratified, non-keratinising squamous epithelium with minimal maturation and diffuse nuclear atypia extending to the superficial layers (A). Neoplastic cells exhibit diffuse, block-type p16 immunopositivity in more than 70% of cells (B).
Figure 7. Sarcomatoid squamous cell carcinoma of the larynx. Low-power view shows a polypoid lesion (A). Higher-power view demonstrates dysplastic surface epithelium overlying spindle and pleomorphic cells (B). Immunohistochemistry highlights scattered cytokeratin-positive cells (C) with absence of nuclear p40 in the spindle component (D).
Figure 8. Laryngeal adenosquamous carcinoma composed of two spatially distinct components with divergent differentiation and overlying dysplastic surface epithelium (A). On the left, nests of poorly differentiated squamous cells show strong p40 positivity, while on the right, a gland-forming component lacks keratinisation and demonstrates only focal or incomplete p40 immunoreactivity (A,B).
References
- Global Cancer Observatory. World Health Organization
- O’Neill R, Hintze J, Sharifah A. Non-conventional laryngeal malignancies: a multicentre review of management and outcomes. Eur Arch Otorhinolaryngol. 2023;280:3383-3392. doi:https://doi.org/10.1007/s00405-023-07937-7
- Milano A. Cancer of the larynx-20-year comparative survival and mortality analysis by age, sex, race, stage, grade, cohort entry time-period, disease duration and ICD-O-3 topographic primary sites-codes C32.0-9: a systematic review of 43,103 cases for diagnosis years 1975-2017: (NCI SEER*Stat 8.3.9). J Insur Med. 2024;51:92-110. doi:https://doi.org/10.17849/insm-51-2-92-110.1
- Zidar N, Thompson L, Agaimy A. The impact of histopathology on prognosis of squamous cell carcinoma of the larynx: can we do better?. Virchows Arch. 2025;487:13-32. doi:https://doi.org/10.1007/s00428-025-04082-w
- Lewis J. Not your usual cancer case: variants of laryngeal squamous cell carcinoma. Head Neck Pathol. 2011;5:23-30. doi:https://doi.org/10.1007/s12105-010-0232-0
- Hashibe M, Brennan P, Benhamou S. Alcohol drinking in never users of tobacco, cigarette smoking in never drinkers, and the risk of head and neck cancer: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. J Natl Cancer Inst. 2007;99:777-789. doi:https://doi.org/10.1093/jnci/djk179
- Scott J. Artificial insemination by donor. Br Med J. 1973;2. doi:https://doi.org/10.1136/bmj.2.5869.781
- Pandey M, Chandramohan K, Thomas G. Soft tissue sarcoma of the head and neck region in adults. Int J Oral Maxillofac Surg. 2003;32:43-48. doi:https://doi.org/10.1054/ijom.2001.0218
- Chiesa-Estomba C, Barillari M, Mayo-Yáñez M. Non-squamous cell carcinoma of the larynx: a state-of-the-art review. J Pers Med. 2023;13. doi:https://doi.org/10.3390/jpm13071084
- Gélinas J, Manoukian J, Côté A. Lung involvement in juvenile onset recurrent respiratory papillomatosis: a systematic review of the literature. Int J Pediatr Otorhinolaryngol. 2008;72:433-452. doi:https://doi.org/10.1016/j.ijporl.2007.12.003
- Syrjänen S. Current concepts on human papillomavirus infections in children. APMIS. 2010;118:494-509. doi:https://doi.org/10.1111/j.1600-0463.2010.02620.x
- Niyibizi J, Rodier C, Wassef M. Risk factors for the development and severity of juvenile-onset recurrent respiratory papillomatosis: a systematic review. Int J Pediatr Otorhinolaryngol. 2014;78:186-197. doi:https://doi.org/10.1016/j.ijporl.2013.11.036
- Derkay C, Wiatrak B. Recurrent respiratory papillomatosis: a review. Laryngoscope. 2008;118:1236-1247. doi:https://doi.org/10.1097/MLG.0b013e31816a7135
- Carifi M, Napolitano D, Morandi M. Recurrent respiratory papillomatosis: current and future perspectives. Ther Clin Risk Manag. 2015;11:731-738. doi:https://doi.org/10.2147/TCRM.S81825
- Gale N, Poljak M, Kambic V. Laryngeal papillomatosis: molecular, histopathological, and clinical evaluation. Virchows Arch. 1994;425:291-295. doi:https://doi.org/10.1007/BF00196152
- Wiatrak B, Wiatrak D, Broker T. Recurrent respiratory papillomatosis: a longitudinal study comparing severity associated with human papilloma viral types 6 and 11 and other risk factors in a large pediatric population. Laryngoscope. 2004;114:1-23. doi:https://doi.org/10.1097/01.mlg.000148224.83491.0f
- Soloperto D, Gazzini S, Cerullo R. Molecular mechanisms of carcinogenesis in pediatric airways tumors. Int J Mol Sci. 2023;24. doi:https://doi.org/10.3390/ijms24032195
- Gluvajić D, Hošnjak L, Stegel V. Risk factors for the development of high-grade dysplasia and carcinoma in patients with laryngeal squamous cell papillomas: large retrospective cohort study. Head Neck. Published online 2020. doi:https://doi.org/10.1002/hed.26560
- Katsenos S, Becker H. Recurrent respiratory papillomatosis: a rare chronic disease, difficult to treat, with potential to lung cancer transformation: apropos of two cases and a brief literature review. Case Rep Oncol. 2011;4:162-171. doi:https://doi.org/10.1159/000327094
- Kanazawa T, Fukushima N, Imayoshi S. Rare case of malignant transformation of recurrent respiratory papillomatosis associated with human papillomavirus type 6 infection and p53 overexpression. Springerplus. 2013;2. doi:https://doi.org/10.1186/2193-1801-2-153
- Omland T, Lie K, Akre H. Recurrent respiratory papillomatosis: HPV genotypes and risk of high-grade laryngeal neoplasia. PLoS One. 2014;9. doi:https://doi.org/10.1371/journal.pone.0099114
- Novakovic D, Cheng A, Zurynski Y. A prospective study of the incidence of juvenile-onset recurrent respiratory papillomatosis after implementation of a national HPV vaccination program. J Infect Dis. 2018;217:208-212. doi:https://doi.org/10.1093/infdis/jix498
- Hočevar-Boltežar I, Matičič M, Sereg-Bahar M. Human papilloma virus vaccination in patients with an aggressive course of recurrent respiratory papillomatosis. Eur Arch Otorhinolaryngol. 2014;271:3255-3262. doi:https://doi.org/10.1007/s00405-014-3143-y
- Gale N, Zidar N, Poljak M. Current views and perspectives on classification of squamous intraepithelial lesions of the head and neck. Head Neck Pathol. 2014;8:16-23. doi:https://doi.org/10.1007/s12105-014-0530-z
- Tanaka S, Morita Y, Fujita T. Clinicopathological characteristics of abnormal micro-lesions at the oro-hypopharynx detected by a magnifying narrow band imaging system. Dig Endosc. 2012;24:100-109. doi:https://doi.org/10.1111/j.1443-1661.2011.01177.x
- Junker K. Pathology of tracheal tumors. Thorac Surg Clin. 2014;24:7-11. doi:https://doi.org/10.1016/j.thorsurg.2013.09.008
- Odell E, Eckel H, Simo R. European Laryngological Society position paper on laryngeal dysplasia Part I: aetiology and pathological classification. Eur Arch Otorhinolaryngol. 2021;278:1717-1722. doi:https://doi.org/10.1007/s00405-020-06403-y
- Gale N, Michaels L, Luzar B. Current review on squamous intraepithelial lesions of the larynx. Histopathology. 2009;54:639-656. doi:https://doi.org/10.1111/j.1365-2559.2008.03111.x
- Sadri M, McMahon J, Parker A. Laryngeal dysplasia: aetiology and molecular biology. J Laryngol Otol. 2006;120:170-177. doi:https://doi.org/10.1017/S0022215105005360
- Vaezi M, Qadeer M, Lopez R. Laryngeal cancer and gastroesophageal reflux disease: a case-control study. Am J Med. 2006;119:768-776. doi:https://doi.org/10.1016/j.amjmed.2006.01.019
- Lewin J, Gillenwater A, Garrett J. Characterization of laryngopharyngeal reflux in patients with premalignant or early carcinomas of the larynx. Cancer. 2003;97:1010-1014. doi:https://doi.org/10.1002/cncr.11158
- Duray A, Descamps G, Arafa M. High incidence of high-risk HPV in benign and malignant lesions of the larynx. Int J Oncol. 2011;39:51-59. doi:https://doi.org/10.3892/ijo.2011.1031
- Mooren J, Gültekin S, Straetmans J. P16(INK4A) immunostaining is a strong indicator for high-risk-HPV-associated oropharyngeal carcinomas and dysplasias, but is unreliable to predict low-risk-HPV-infection in head and neck papillomas and laryngeal dysplasias. Int J Cancer. 2014;134:2108-2117. doi:https://doi.org/10.1002/ijc.28534
- Pagliuca G, Martellucci S, Degener A. Role of Human Papillomavirus in the pathogenesis of laryngeal dysplasia. Otolaryngol Head Neck Surg. 2014;150:1018-1023. doi:https://doi.org/10.1177/0194599814525749
- Zhang L, Lewis J, El-Mofty S. Nonkeratinizing squamous cell carcinoma in situ of the upper aerodigestive tract: an HPV-related entity. Head Neck Pathol. 2017;11:152-161. doi:https://doi.org/10.1007/s12105-016-0749-y
- van Hulst A, Kroon W, van der Linden E. Grade of dysplasia and malignant transformation in adults with premalignant laryngeal lesions. Head Neck. 2016;38:E2284-E2290. doi:https://doi.org/10.1002/hed.24185
- McLaren K, Burnett R, Goodlad J. Consistency of histopathological reporting of laryngeal dysplasia. The Scottish Pathology Consistency Group. Histopathology. 2000;37:460-463. doi:https://doi.org/10.1046/j.1365-2559.2000.00998.x
- Sarioglu S, Cakalagaoglu F, Elagoz S. Inter-observer agreement in laryngeal pre-neoplastic lesions. Head Neck Pathol. 2010;4:276-280. doi:https://doi.org/10.1007/s12105-010-0208-0
- Fleskens S, Bergshoeff V, Voogd A. Interobserver variability of laryngeal mucosal premalignant lesions: a histopathological evaluation. Mod Pathol. 2011;24:892-898. doi:https://doi.org/10.1038/modpathol.2011.50
- Gale N, Cardesa A, Hernandez-Prera J. Laryngeal dysplasia: persisting dilemmas, disagreements and unsolved problems – A short review. Head Neck Pathol. 2020;14:1046-1051. doi:https://doi.org/10.1007/s12105-020-01149-9
- Hellquist H, Ferlito A, Mäkitie A. Developing classifications of laryngeal dysplasia: the historical basis. Adv Ther. 2020;37:2667-2677. doi:https://doi.org/10.1007/s12325-020-01348-4
- Gale N, Blagus R, El-Mofty S. Evaluation of a new grading system for laryngeal squamous intraepithelial lesions – A proposed unified classification. Histopathology. 2014;65:456-464. doi:https://doi.org/10.1111/his.12427
- Zhang H, Liu H. Is severe dysplasia the same lesion as carcinoma in situ? 10-year follow-up of laryngeal precancerous lesions. Acta Otolaryngol. 2012;132:325-328. doi:https://doi.org/10.3109/00016489.2011.642812
- Siegel R, Miller K, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70:7-30. doi:https://doi.org/10.3322/caac.21590
- Aupérin A. Epidemiology of head and neck cancers: an update. Curr Opin Oncol. 2020;32:178-186. doi:https://doi.org/10.1097/CCO.0000000000000629
- Lin L, Yan L, Liu Y. Incidence and death in 29 cancer groups in 2017 and trend analysis from 1990 to 2017 from the Global Burden of Disease Study. J Hematol Oncol. 2019;12. doi:https://doi.org/10.1186/s13045-019-0783-9
- Smith R, Caulk R, Frazell E. Revision of the clinical staging system for cancer of the larynx. Cancer. 1973;31:72-80. doi:https://doi.org/10.1002/1097-0142(197301)31:1%3C72::aid-cncr2820310110%3E3.0.co;2-v
- Patel T, Echanique K, Yip C. Supraglottic squamous cell carcinoma: a population-based study of 22,675 cases. Laryngoscope. 2019;129:1822-1827. doi:https://doi.org/10.1002/lary.27592
- Tomik J, Składzien J, Modrzejewski M. Evaluation of cervical lymph node metastasis of 1400 patients with cancer of the larynx. Auris Nasus Larynx. 2001;28:233-240. doi:https://doi.org/10.1016/s0385-8146(00)00116-4
- Marchiano E, Patel D, Patel T. Subglottic squamous cell carcinoma: a population-based study of 889 cases. Otolaryngol Head Neck Surg. 2016;154:315-321. doi:https://doi.org/10.1177/0194599815618190
- Verro B, Fiumara S, Saraniti G. Laryngeal cancer in women: unveiling gender-specific risk factors, treatment challenges, and survival disparities. Curr Oncol. 2024;32. doi:https://doi.org/10.3390/curroncol32010019
- Di Credico G, Edefonti V, Polesel J. Joint effects of intensity and duration of cigarette smoking on the risk of head and neck cancer: a bivariate spline model approach. Oral Oncol. 2019;94:47-57. doi:https://doi.org/10.1016/j.oraloncology.2019.05.006
- Parsel S, Wu E, Riley C. Gastroesophageal and laryngopharyngeal reflux associated with laryngeal malignancy: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2019;17:1253-1264. doi:https://doi.org/10.1016/j.cgh.2018.10.028
- Eells A, Mackintosh C, Marks L. Gastroesophageal reflux disease and head and neck cancers: a systematic review and meta-analysis. Am J Otolaryngol. 2020;41. doi:https://doi.org/10.1016/j.amjoto.2020.102653
- Lewis J, Ukpo O, Ma X. Transcriptionally-active high-risk human papillomavirus is rare in oral cavity and laryngeal/hypopharyngeal squamous cell carcinomas – A tissue microarray study utilizing E6/E7 mRNA in situ hybridization. Histopathology. 2012;60:982-991. doi:https://doi.org/10.1111/j.1365-2559.2011.04169.x
- Barsouk A, Aluru J, Rawla P. Epidemiology, risk factors, and prevention of head and neck squamous cell carcinoma. Med Sci (Basel). 2023;11. doi:https://doi.org/10.3390/medsci11020042
- Forsyth A, Camilon P, Tracy L. Pediatric laryngeal tumors and demographics, management, and survival in laryngeal squamous cell carcinoma. Int J Pediatr Otorhinolaryngol. 2021;140. doi:https://doi.org/10.1016/j.ijporl.2020.110507
- Bayan S, Faquin W, Zeitels S. Glottic carcinoma in young patients. Ann Otol Rhinol Laryngol. 2019;128:25S-32S. doi:https://doi.org/10.1177/0003489418818852
- Dombrowski N, Wolter N, Irace A. Squamous cell carcinoma of the head and neck in children. Int J Pediatr Otorhinolaryngol. 2019;117:131-137. doi:https://doi.org/10.1016/j.ijporl.2018.11.019
- Poeta M, Manola J, Goldwasser M. TP53 mutations and survival in squamous-cell carcinoma of the head and neck. N Engl J Med. 2007;357:2552-2561. doi:https://doi.org/10.1056/NEJMoa073770
- MacMillan C, Kapadia S, Finkelstein S. Lymphoepithelial carcinoma of the larynx and hypopharynx: study of eight cases with relationship to Epstein-Barr virus and p53 gene alterations, and review of the literature. Hum Pathol. 1996;27:1172-1179. doi:https://doi.org/10.1016/s0046-8177(96)90311-1
- Qian W, Zhu G, Wang Y. Multi-modality management for loco-regionally advanced laryngeal and hypopharyngeal cancer: balancing the benefit of efficacy and functional preservation. Med Oncol. 2014;31. doi:https://doi.org/10.1007/s12032-014-0178-2
- Skarsgard D, Groome P, Mackillop W. Cancers of the upper aerodigestive tract in Ontario, Canada, and the United States. Cancer. 2000;88:1728-1738. doi:https://doi.org/10.1002/(sici)1097-0142(20000401)88:7%3C1728::aid-cncr29%3E3.0.co;2-7
- Bradford C, Ferlito A, Devaney K. Prognostic factors in laryngeal squamous cell carcinoma. Laryngoscope Investig Otolaryngol. 2020;5:74-81. doi:https://doi.org/10.1002/lio2.353
- Sethi S, Lu M, Kapke A. Patient and tumor factors at diagnosis in a multi-ethnic primary head and neck squamous cell carcinoma cohort. J Surg Oncol. 2009;99:104-108. doi:https://doi.org/10.1002/jso.21190
- Lee K, Chuang S. The nonsurgical management of early stage (T1/2 N0 M0) laryngeal cancer: a population analysis. Oral Surg Oral Med Oral Pathol Oral Radiol. 2020;130:18-24. doi:https://doi.org/10.1016/j.oooo.2020.01.006
- Wang Z, Zeng Q, Li Y. Extranodal extension as an independent prognostic factor in laryngeal squamous cell carcinoma patients. J Cancer. 2020;11:7196-7201. doi:https://doi.org/10.7150/jca.47700
- Tulli M, Re M, Bondi S. The prognostic value of anterior commissure involvement in T1 glottic cancer: a systematic review and meta-analysis. Laryngoscope. 2020;130:1932-1940. doi:https://doi.org/10.1002/lary.28395
- Boxberg M, Kuhn P, Reiser M. Tumor budding and cell nest size are highly prognostic in laryngeal and hypopharyngeal squamous cell carcinoma: further evidence for a unified histopathologic grading system for squamous cell carcinomas of the upper aerodigestive tract. Am J Surg Pathol. 2019;43:303-313. doi:https://doi.org/10.1097/PAS.0000000000001178
- Mäkitie A, Almangush A, Rodrigo J. Hallmarks of cancer: tumor budding as a sign of invasion and metastasis in head and neck cancer. Head Neck. 2019;41:3712-3718. doi:https://doi.org/10.1002/hed.25872
- Brandwein-Gensler M, Smith R, Wang B. Validation of the histologic risk model in a new cohort of patients with head and neck squamous cell carcinoma. Am J Surg Pathol. 2010;34:676-688. doi:https://doi.org/10.1097/PAS.0b013e3181d95c37
- Fletcher K, Gal T, Ebelhar A. Prognostic indicators and survival in salvage surgery for laryngeal cancer. Head Neck. 2017;39:2021-2026. doi:https://doi.org/10.1002/hed.24860
- Singh A, Qayyumi B, Chaturvedi P. An update on surgical margins in the head neck squamous cell carcinoma: assessment, clinical outcome, and future directions. Curr Oncol Rep. 2020;22. doi:https://doi.org/10.1007/s11912-020-00942-7
- Hendriksma M, Montagne M, Langeveld T. Evaluation of surgical margin status in patients with early glottic cancer (Tis-T2) treated with transoral CO2 laser microsurgery, on local control. Eur Arch Otorhinolaryngol. 2018;275:2333-2340. doi:https://doi.org/10.1007/s00405-018-5070-9
- Li R, Yu S, Zhu W. Studying the impact of young age on prognosis and treatment in laryngeal squamous cell carcinomas using the SEER database. PeerJ. 2019;7. doi:https://doi.org/10.7717/peerj.7368
- Mulcahy C, Mohamed A. Age-adjusted comorbidity and survival in locally advanced laryngeal cancer. Head Neck. 2018;40:2060-2069. doi:https://doi.org/10.1002/hed.25200
- Fong P, Tan S, Lim D. Association of clinical factors with survival outcomes in laryngeal squamous cell carcinoma (LSCC). PLoS One. 2019;14. doi:https://doi.org/10.1371/journal.pone.0224665
- Chen S, Li S, Shi D. Expression of PD-1/PD-L1 in head and neck squamous cell carcinoma and its clinical significance. Int J Biol Markers. 2019;34:398-405. doi:https://doi.org/10.1177/1724600819884722
- Burtness B, Harrington K, Greil R. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet. 2019;394:1915-1928. doi:https://doi.org/10.1016/S0140-6736(19)32591-7
- Wain S, Kier R, Vollmer R. Basaloid-squamous carcinoma of the tongue, hypopharynx, and larynx: report of 10 cases. Hum Pathol. 1986;17:1158-1166. doi:https://doi.org/10.1016/s0046-8177(86)80422-1
- Begum S, Westra W. Basaloid squamous cell carcinoma of the head and neck is a mixed variant that can be further resolved by HPV status. Am J Surg Pathol. 2008;32:1044-1050. doi:https://doi.org/10.1097/PAS.0b013e31816380ec
- Chernock R, Lewis J, Zhang Q. Human papillomavirus-positive basaloid squamous cell carcinomas of the upper aerodigestive tract: a distinct clinicopathologic and molecular subtype of basaloid squamous cell carcinoma. Hum Pathol. 2010;41:1016-1023. doi:https://doi.org/10.1016/j.humpath.2009.11.015
- Rooper L, McCuiston A, Westra W. SOX10 immunoexpression in basaloid squamous cell carcinomas: a diagnostic pitfall for ruling out salivary differentiation. Head Neck Pathol. 2019;13:543-547. doi:https://doi.org/10.1007/s12105-018-0990-7
- Winzenburg S, Niehans G, George E. Basaloid squamous carcinoma: a clinical comparison of two histologic types with poorly differentiated squamous cell carcinoma. Otolaryngol Head Neck Surg. 1998;119:471-475. doi:https://doi.org/10.1016/S0194-5998(98)70104-4
- Banks E, Frierson H, Mills S. Basaloid squamous cell carcinoma of the head and neck. A clinicopathologic and immunohistochemical study of 40 cases. Am J Surg Pathol. 1992;16:939-946. doi:https://doi.org/10.1097/00000478-199210000-00003
- Linton O, Moore M, Brigance J. Prognostic significance of basaloid squamous cell carcinoma in head and neck cancer. JAMA Otolaryngol Head Neck Surg. 2013;139:1306-1311. doi:https://doi.org/10.1001/jamaoto.2013.5308
- Fritsch V, Lentsch E. Basaloid squamous cell carcinoma of the larynx: analysis of 145 cases with comparison to conventional squamous cell carcinoma. Head Neck. 2014;36:164-170. doi:https://doi.org/10.1002/hed.23286
- Fritsch V, Lentsch E. Basaloid squamous cell carcinoma of the head and neck: location means everything. J Surg Oncol. 2014;109:616-622. doi:https://doi.org/10.1002/jso.23536
- Kraus F, Perezmesa C. Verrucous carcinoma. Clinical and pathologic study of 105 cases involving oral cavity, larynx and genitalia. Cancer. 1966;19:26-38. doi:https://doi.org/10.1002/1097-0142(196601)19:1%3C26::aid-cncr2820190103%3E3.0.co;2-l
- Koch B, Trask D, Hoffman H. National survey of head and neck verrucous carcinoma: patterns of presentation, care, and outcome. Cancer. 2001;92:110-120. doi:https://doi.org/10.1002/1097-0142(20010701)92:1%3C110::aid-cncr1298%3E3.0.co;2-k
- Dubal P, Svider P, Kam D. Laryngeal verrucous carcinoma: a population-based analysis. Otolaryngol Head Neck Surg. 2015;153:799-805. doi:https://doi.org/10.1177/0194599815591981
- Ferlito A, Recher G. Ackerman’s tumor (verrucous carcinoma) of the larynx: a clinicopathologic study of 77 cases. Cancer. 1980;46:1617-1630. doi:https://doi.org/10.1002/1097-0142(19801001)46:7%3C1617::aid-cncr2820460722%3E3.0.co;2-t
- Hod R, Feinmesser R, Shvero J. Carbon dioxide laser cordectomy for verrucous carcinoma of vocal folds. J Laryngol Otol. 2010;124:55-58. doi:https://doi.org/10.1017/S002221510999140X
- López-Amado M, García-Caballero T, Lozano-Ramírez A. Human papillomavirus and p53 oncoprotein in verrucous carcinoma of the larynx. J Laryngol Otol. 1996;110:742-747. doi:https://doi.org/10.1017/s0022215100134851
- Odar K, Kocjan B, Hošnjak L. Verrucous carcinoma of the head and neck - not a human papillomavirus-related tumour?. J Cell Mol Med. 2014;18:635-645. doi:https://doi.org/10.1111/jcmm.12211
- Patel K, Chernock R, Zhang T. Verrucous carcinomas of the head and neck, including those with associated squamous cell carcinoma, lack transcriptionally active high-risk human papillomavirus. Hum Pathol. 2013;44:2385-2392. doi:https://doi.org/10.1016/j.humpath.2013.07.011
- Echanique K, Desai S, Marchiano E. Laryngeal verrucous carcinoma. Otolaryngol Head Neck Surg. 2017;156:38-45. doi:https://doi.org/10.1177/0194599816662631
- Orvidas L, Olsen K, Lewis J. Verrucous carcinoma of the larynx: a review of 53 patients. Head Neck. 1998;20:197-203. doi:https://doi.org/10.1002/(sici)1097-0347(199805)20:3%3C197::aid-hed3%3E3.0.co;2-w
- Wang N, Huang M, Lv H. Head and neck verrucous carcinoma: a population-based analysis of incidence, treatment, and prognosis. Medicine (Baltimore). 2020;99. doi:https://doi.org/10.1097/MD.0000000000018660
- Milford C, O’Flynn P. Management of verrucous carcinoma of the larynx. Clin Otolaryngol Allied Sci. 1991;16:160-162. doi:https://doi.org/10.1111/j.1365-2273.1991.tb01968.x
- Ferlito A, Rinaldo A, Mannarà G. Is primary radiotherapy an appropriate option for the treatment of verrucous carcinoma of the head and neck?. J Laryngol Otol. 1998;112:132-139. doi:https://doi.org/10.1017/s0022215100140137
- López F, Williams M, Cardesa A. How phenotype guides management of non-conventional squamous cell carcinomas of the larynx?. Eur Arch Otorhinolaryngol. 2017;274:2709-2726. doi:https://doi.org/10.1007/s00405-017-4533-8
- Jo V, Mills S, Stoler M. Papillary squamous cell carcinoma of the head and neck: frequent association with human papillomavirus infection and invasive carcinoma. Am J Surg Pathol. 2009;33:1720-1724. doi:https://doi.org/10.1097/PAS.0b013e3181b6d8e6
- Suarez P, Adler-Storthz K, Luna M. Papillary squamous cell carcinomas of the upper aerodigestive tract: a clinicopathologic and molecular study. Head Neck. 2000;22:360-368. doi:https://doi.org/10.1002/1097-0347(200007)22:4%3C360::aid-hed8%3E3.0.co;2-w
- Colby C, Klein A. Papillary squamous cell carcinoma of the larynx. Ear Nose Throat J. 2011;90:E13-E15. doi:https://doi.org/10.1177/014556131109000817
- Thompson L, Wenig B, Heffner D. Exophytic and papillary squamous cell carcinomas of the larynx: a clinicopathologic series of 104 cases. Otolaryngol Head Neck Surg. 1999;120:718-724. doi:https://doi.org/10.1053/hn.1999.v120.a92773
- Dutta R, Husain Q, Kam D. Laryngeal papillary squamous cell carcinoma: a population-based analysis of incidence and survival. Otolaryngol Head Neck Surg. 2015;153:54-59. doi:https://doi.org/10.1177/0194599815581613
- Thompson L, Wieneke J, Miettinen M. Spindle cell (sarcomatoid) carcinomas of the larynx: a clinicopathologic study of 187 cases. Am J Surg Pathol. 2002;26:153-170. doi:https://doi.org/10.1097/00000478-200202000-00002
- Gerry D, Fritsch V, Lentsch E. Spindle cell carcinoma of the upper aerodigestive tract: an analysis of 341 cases with comparison to conventional squamous cell carcinoma. Ann Otol Rhinol Laryngol. 2014;123:576-583. doi:https://doi.org/10.1177/0003489414525337
- Watson R, Chernock R, Wang X. Spindle cell carcinomas of the head and neck rarely harbor transcriptionally-active human papillomavirus. Head Neck Pathol. 2013;7:250-257. doi:https://doi.org/10.1007/s12105-013-0438-z
- Olsen K, Lewis J, Suman V. Spindle cell carcinoma of the larynx and hypopharynx. Otolaryngol Head Neck Surg. 1997;116:47-52. doi:https://doi.org/10.1016/S0194-59989770351-6
- Dubal P, Marchiano E, Kam D. Laryngeal spindle cell carcinoma: a population-based analysis of incidence and survival. Laryngoscope. 2015;125:2709-2714. doi:https://doi.org/10.1002/lary.25383
- Roy S, Purgina B, Seethala R. Spindle cell carcinoma of the larynx with rhabdomyoblastic heterologous element: a rare form of divergent differentiation. Head Neck Pathol. 2013;7:263-267. doi:https://doi.org/10.1007/s12105-012-0402-3
- Elzamly S, Zhu H, Karni R. Spindle cell squamous cell carcinoma of the larynx with malignant osteoid differentiation: a case report and review of literature. Ann Clin Lab Sci. 2021;51:415-421.
- Spector M, Wilson K, Light E. Clinical and pathologic predictors of recurrence and survival in spindle cell squamous cell carcinoma. Otolaryngol Head Neck Surg. 2011;145:242-247. doi:https://doi.org/10.1177/0194599811402167
- Kass J, Lee S, Abberbock S. Adenosquamous carcinoma of the head and neck: molecular analysis using CRTC-MAML FISH and survival comparison with paired conventional squamous cell carcinoma. Laryngoscope. 2015;125:E371-E376. doi:https://doi.org/10.1002/lary.25519
- Dubal P, Unsal A, Echanique K. Laryngeal adenosquamous carcinoma: a population-based perspective. Laryngoscope. 2016;126:858-863. doi:https://doi.org/10.1002/lary.25704
- Thompson L. Laryngeal dysplasia, squamous cell carcinoma, and variants. Surg Pathol Clin. 2017;10:15-33. doi:https://doi.org/10.1016/j.path.2016.10.003
- Mokhtari S, Mohsenifar Z, Mokhtari S. Diagnostic histological features of metastatic lymph nodes in adenosquamous carcinoma. Pathol Res Pract. 2012;208:360-362. doi:https://doi.org/10.1016/j.prp.2012.04.002
- Alos L, Castillo M, Nadal A. Adenosquamous carcinoma of the head and neck: criteria for diagnosis in a study of 12 cases. Histopathology. 2004;44:570-579. doi:https://doi.org/10.1111/j.1365-2559.2004.01881.x
- Lovato A, Staffieri A, Marino F. Immunohistochemical and HPV-related features of laryngeal adenosquamous carcinoma. Am J Otolaryngol. 2015;36:442-445. doi:https://doi.org/10.1016/j.amjoto.2014.12.007
- Micheau C, Luboinski B, Schwaab G. Lymphoepitheliomas of the larynx (undifferentiated carcinomas of nasopharyngeal type). Clin Otolaryngol Allied Sci. 1979;4:43-48. doi:https://doi.org/10.1111/j.1365-2273.1979.tb01751.x
- Marioni G, Mariuzzi L, Gaio E. Lymphoepithelial carcinoma of the larynx. Acta Otolaryngol. 2002;122:429-434. doi:https://doi.org/10.1080/00016480260000148
- Chan J, Wong E, Ng S. Non-nasopharyngeal head and neck lymphoepithelioma-like carcinoma in the United States: a population-based study. Head Neck. 2016;38:E1294-E1300. doi:https://doi.org/10.1002/hed.24215
- Zbären P, Borisch B, Läng H. Undifferentiated carcinoma of nasopharyngeal type of the laryngopharyngeal region. Otolaryngol Head Neck Surg. 1997;117:688-693. doi:https://doi.org/10.1016/S0194-59989770053-6
- Wenig B. Lymphoepithelial-like carcinomas of the head and neck. Semin Diagn Pathol. 2015;32:74-86. doi:https://doi.org/10.1053/j.semdp.2014.12.004
- Weiss L, Gaffey M, Shibata D. Lymphoepithelioma-like carcinoma and its relationship to Epstein-Barr virus. Am J Clin Pathol. 1991;96:156-158. doi:https://doi.org/10.1093/ajcp/96.2.156
- Iezzoni J, Gaffey M, Weiss L. The role of Epstein-Barr virus in lymphoepithelioma-like carcinomas. Am J Clin Pathol. 1995;103:308-315. doi:https://doi.org/10.1093/ajcp/103.3.308
- Monteiro F, Baldaia H, Ribeiro L. Epstein-Barr Virus-associated with lymphoepithelial carcinoma: a rare tumor of the larynx. Clin Med Insights Ear Nose Throat. 2019;12. doi:https://doi.org/10.1177/1179550619865551
- Bhaumik S, Singh P, Reddy N. Lympho-epithelial carcinoma of the larynx – The big masquerader of squamous cell carcinoma – A case report. Ecancermedicalscience. 2025;19. doi:https://doi.org/10.3332/ecancer.2025.1936
- Dray T, Vargas H, Weidner N. Lymphoepitheliomas of the laryngohypopharynx. Am J Otolaryngol. 1998;19:263-266. doi:https://doi.org/10.1016/s0196-0709(98)90129-6
- Faisal M, Hartenbach S, Schratter A. Lymphoepithelial carcinoma of larynx and hypopharynx: a rare clinicopathological entity. Cancers (Basel). 2020;12. doi:https://doi.org/10.3390/cancers12092431
- Nath J, Sarma G, Das A. Lymphoepithelial carcinoma of the larynx: a clinical report with pooled analysis and review of published cases. J Cancer Res Ther. 2023;19:S466-S471. doi:https://doi.org/10.4103/jcrt.jcrt_1390_22
- Dubey P, Ha C, Ang K. Nonnasopharyngeal lymphoepithelioma of the head and neck. Cancer. 1998;82:1556-1562. doi:https://doi.org/10.1002/(sici)1097-0142(19980415)82:8%3C1556::aid-cncr18%3E3.0.co;2-3
- Coskun B, Cinar U, Sener B. Lymphoepithelial carcinoma of the larynx. Auris Nasus Larynx. 2005;32:189-193. doi:https://doi.org/10.1016/j.anl.2004.11.014
- Hammas N, Benmansour N, El Alami El Amine M. Lymphoepithelial carcinoma: a case report of a rare tumor of the larynx. BMC Clin Pathol. 2017;17. doi:https://doi.org/10.1186/s12907-017-0061-0
- Wolf G, Fisher S, Hong W. Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. N Engl J Med. 1991;324:1685-1690. doi:https://doi.org/10.1056/NEJM199106133242402
- Forastiere A, Zhang Q, Weber R. Long-term results of RTOG 91-11: a comparison of three nonsurgical treatment strategies to preserve the larynx in patients with locally advanced larynx cancer. J Clin Oncol. 2013;31:845-852. doi:https://doi.org/10.1200/JCO.2012.43.6097
- Pointreau Y, Garaud P, Chapet S. Randomized trial of induction chemotherapy with cisplatin and 5-fluorouracil with or without docetaxel for larynx preservation. J Natl Cancer Inst. 2009;101:498-506. doi:https://doi.org/10.1093/jnci/djp007
- Lefebvre J, Pointreau Y, Rolland F. Induction chemotherapy followed by either chemoradiotherapy or bioradiotherapy for larynx preservation: the TREMPLIN randomized phase II study. J Clin Oncol. 2013;31:853-859. doi:https://doi.org/10.1200/JCO.2012.42.3988
- Dietz A, Wichmann G, Kuhnt T. Induction chemotherapy (IC) followed by radiotherapy (RT) versus cetuximab plus IC and RT in advanced laryngeal/hypopharyngeal cancer resectable only by total laryngectomy-final results of the larynx organ preservation trial DeLOS-II. Ann Oncol. 2018;29:2105-2114. doi:https://doi.org/10.1093/annonc/mdy332
- Harrington K, Burtness B, Greil R. Pembrolizumab with or without chemotherapy in recurrent or metastatic head and neck squamous cell carcinoma: updated results of the phase III KEYNOTE-048 study. J Clin Oncol. 2023;41:790-802. doi:https://doi.org/10.1200/JCO.21.02508
- Verro B, Saraniti G, Ottoveggio G. Cancer and immune response: the role of PD-1/PD-L1 checkpoint in laryngeal carcinoma. Preliminary results. Eur Arch Otorhinolaryngol. 2024;281:5411-5417. doi:https://doi.org/10.1007/s00405-024-08822-7
- Saâda-Bouzid E, Defaucheux C, Karabajakian A. Hyperprogression during anti-PD-1/PD-L1 therapy in patients with recurrent and/or metastatic head and neck squamous cell carcinoma. Ann Oncol. 2017;28:1605-1611. doi:https://doi.org/10.1093/annonc/mdx178
- Taylor M, Lee C, Makker V. Phase IB/II trial of lenvatinib plus pembrolizumab in patients with advanced renal cell carcinoma, endometrial cancer, and other selected advanced solid tumors. J Clin Oncol. 2020;38:1154-1163. doi:https://doi.org/10.1200/JCO.19.01598
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 665 times
- PDF downloaded - 79 times