Annual congress report
Vol. 46: 112 TH CONGRESS SIOECHCF - OFFICIAL REPORT 2026
Post-laryngectomy videofluoroscopic assessment in relation to olfactory rehabilitation through the physiological olfactory recovery technique
Summary
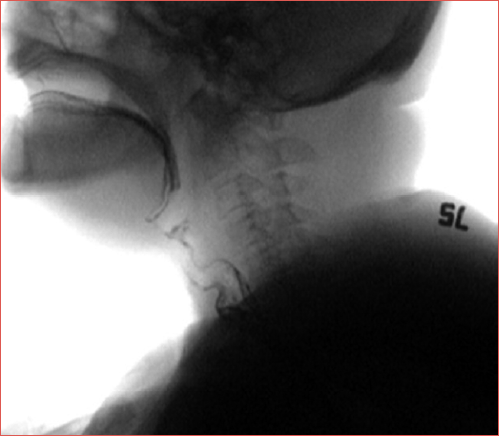
Cover Image
Objective. To correlate the anatomo-physiological characteristics of post-laryngectomy changes, assessed by videofluoroscopy, with the outcome and modalities of olfactory rehabilitation using the physiological olfactory recovery technique (PORT).
Materials and methods. From 2019 to 2021, a prospective observational study was conducted at the Department of Otolaryngology-Head and Neck Surgery of Ospedale del Mare, Naples, Italy, on 31 patients who had undergone total laryngectomy with primary placement of a tracheo-oesophageal voice prosthesis. All patients completed a proprioceptive training programme with a speech-language pathologist and learned the PORT method. At the end of the 10-session rehabilitation protocol, all participants demonstrated significant improvement in olfactory perception, which was maintained at long-term follow-up. During subsequent application of PORT in selected patients, notable inter-patient differences emerged in both the modality and timing of response to rehabilitation. This prompted an anatomo-physiological investigation of the post-laryngectomy changes to objectify these variable outcomes. As part of an ongoing collaborative project between the Otolaryngology and Radiology Units aimed at monitoring swallowing and phonatory function in laryngectomized patients, videofluoroscopic examinations were analysed. A total of 31 videofluoroscopic studies performed between February and October 2022 were reviewed.
Results. Differences in patient responses to PORT correlated with individual anatomo-physiological variations in the amount and distribution of air reaching the proximal oesophagus during phonation − defined as the phonatory air bubble (PAB) − as well as with differences in the elasticity of the anatomical district examined. Five distinct types of proximal oesophageal PABs were identified, classified according to post-surgical anatomical characteristics and functional alterations related to adjuvant therapy, particularly radiation-induced fibrosis.
Conclusions. PORT is an effective olfactory rehabilitation technique for laryngectomised patients with a trachea-oesophageal voice prosthesis, including those with complex anatomo-physiological conditions. Accurate interpretation of post-laryngectomy changes is essential for evaluating treatment efficacy: 28 of the 31 patients evaluated physiologically recovered the daily olfactory sniffing manoeuvre, although with variable modalities and timing. Overall, PORT represents a widely applicable and effective method for olfactory rehabilitation in the vast majority of patients with a tracheo-oesophageal voice prosthesis after total laryngectomy.
Introduction
Among all cancer types, laryngeal tumours rank as the 20th most common for incidence, the 18th for prevalence and mortality, and account for 0.8%, 1.4%, and 1.3% of the above mentioned cancer-related events, respectively 1. Over the most recent decades, the development of modular surgical techniques combined with chemotherapy (ChT) and radiotherapy (RT) aimed at organ preservation has reduced the indications for primary total laryngectomy (TL). Nevertheless, this procedure remains the primary surgical approach for advanced laryngeal carcinomas that are not suitable for conservative strategies or demonstrate poor response to them 2. The 5-year disease-specific survival (DSS) rate after salvage TL ranges between 48% and 63% 3,4.
TL results in a complete and permanent separation of the upper and lower airways, with significant consequences for health-related quality of life (HRQoL), including loss of voice, loss of smell, and inability to warm, humidify, and filter inhaled air 5. Breathing through the tracheostoma eliminates nasal airflow and induces progressive atrophy of the nasal mucosa, olfactory epithelium, and/or the olfactory bulb 6,7. The absence of airflow from the nasopharynx to the trachea impairs both orthonasal olfaction (entry of odourants through the nostrils) and retronasal olfaction (passage of odourants from the oropharynx through the nasopharynx and choanae to the olfactory cleft and neuro-olfactory epithelium). This can lead to appetite loss, weight loss, and psychosocial difficulties that negatively affect HRQoL 8,9. As demonstrated by Hanna et al. 5, olfactory loss directly interferes with daily activities involving odour perception.
Despite increasing evidence supporting the effectiveness of olfactory rehabilitation techniques 10,11, their application in clinical practice remains limited. Recently, a new method – the physiological olfactory recovery technique (PORT) 12 – has been introduced as a “physiological” approach to restore both orthonasal and retronasal olfaction. The present study aims to assess the effectiveness of PORT, including its applicability in patients in whom post-laryngectomy changes and neo-physiology may be particularly complex.
Materials and methods
This case-control study included patients who underwent TL with primary placement of a tracheo-oesophageal voice prosthesis (TEP) for advanced laryngeal carcinoma at the Department of Otolaryngology-Head and Neck Surgery of Ospedale del Mare in Naples, Italy. Each patient completed the PORT-based olfactory rehabilitation programme, structured in 10 sessions, and underwent videofluoroscopic assessment of post-laryngectomy anatomical changes. Some patients required an additional 10-session integrative speech therapy programme to complete rehabilitation.
Clinical assessment (history, physical examination, questionnaires) was performed by an Otolaryngologist; olfactory assessment was conducted together by the Otolaryngologist and Speech-Language Pathologist; videofluoroscopy was conducted together by the Radiologist and Speech-Language Pathologist.
Specific inclusion and exclusion criteria were established for patient recruitment.
Inclusion criteria: patients > 18 years old submitted to TL at least 2 months before enrolment; acquisition of trachea-oesophageal voice through a voice rehabilitation programme; autonomous daily management of the trachea-oesophageal prosthesis.
Exclusion criteria: dysfunctional or obstructive swallowing patterns; significant nasal obstruction at nasal endoscopy (e.g., septal deviation, inferior turbinate hypertrophy, olfactory cleft obstruction); history of sinonasal disease and/or olfactory dysfunction; oral motor impairment or neurological abnormalities; (C)RT within the previous 6 months or ongoing treatment.
All subjects enrolled underwent ENT evaluation to rule out nasal obstruction, as well as a speech-language evaluation to confirm autonomous management of the trachea-oesophageal prosthesis and suitability for PORT.
Olfaction was evaluated using subjective olfactometry with Sniffin’ Sticks 13. Patients were classified as: “smellers”, score 9-16 (mild hyposmia = 9-10; normosmia = 11-16); “non-smellers”, score 0-8 (anosmia = 0-5; hyposmia = 6-8) 14.
Additionally, 2 questionnaires were administered: the Chemosensory Complaints Score (CCS) for subjective evaluation of smell and taste 15 and the University of Washington Quality of Life questionnaire – version 4 (UW-QoL v4) for HRQoL assessment 16.
PORT rehabilitation protocol guides patients through a proprioceptive programme with 2 distinct components: orthonasal and retronasal olfactory rehabilitation. The programme consists of 10 sessions: 8 bi-weekly sessions (the first individual, the remaining in small groups of 3-5 patients) and 2 follow-up sessions at 15-day intervals. Sensory stimulation includes 2 phases: identification (4 choices) and recognition (6 fixed odours plus new ones added at each session).
The orthonasal olfaction rehabilitation, applicable to TEP and non-TEP patients, instructs patients to perform an inspiratory manoeuvre with the lips and tracheostoma sealed before sniffing with the stoma closed. During inspiration, diaphragmatic contraction lowers intrathoracic pressure, and the resulting negative oesophageal pressure draws air from the nasal cavities into the oesophagus. To facilitate acquisition, this manoeuvre is objectified by having the patient “inhale” methylene blue-coloured water through a straw placed in one nostril, with lips and tracheostoma sealed. The upward movement of the coloured liquid demonstrates successful orthonasal airflow.
The retronasal olfaction rehabilitation is indicated exclusively for TEP patients, exploiting the unidirectional valve mechanism of the prosthesis. Patients first perform a deep inhalation while sniffing with an open stoma, followed by exhalation with the stoma and mouth sealed. This directs airflow through the voice prosthesis toward the nasal cavities. Initially, patients practice this manoeuvre using a straw; the appearance of bubbles in a glass of water confirms effective exhalation.
PORT seeks to restore pseudo-physiological conditions by re-establishing nasal airflow, enabling odorant molecules to reach the olfactory epithelium. After successful acquisition, patients can perceive odours with the stoma closed.
All patients, upon completing the standard rehabilitation program, subsequently underwent a dynamic radiologic assessment of the entire swallowing act using videofluoroscopy. For the cine-videofluoroscopic study of swallowing, barium meals of different consistencies were administered: semiliquid bolus (5 mL Ba 240%), semisolid bolus (one medium spoon, 14 g, of a mixture composed of 75 g of fruit mousse + one medium spoon of barium powder), solid bolus (rusk dipped in liquid barium), and liquid bolus (5 mL Ba 60%). The examination was performed in the presence of a dedicated speech language pathologist - radiologist team.
For each patient, the anatomy and physiology of the structures involved in both swallowing and phonation were evaluated, as both functions are susceptible to the effects of surgery and adjuvant treatments. In particular, RT may induce stiffness and/or fibrosis 17 at the pharyngoesophageal junction and in its proximal regions, with significant implications for rehabilitation.
Analysis of the cine-videofluoroscopic examinations allowed the identification of 5 distinct types of “proximal oesophageal phonatory air bubble (PAB)”.
This bubble is defined as a dilation of the proximal oesophagus occurring, after tracheal stoma occlusion, due to the passage of air through the trachea-oesophageal voice prosthesis. The different types appeared to be correlated with both anatomical features resulting from surgery and functional alterations associated with adjuvant RT.
Morphology determines the PAB subtype, allowing differentiation between one “regular-morphology PAB” – a drop-shaped dilation with its apex pointing downward (Fig. 1) and 4 types of “irregular-morphology PAB”: a “distally developing bubble” (Fig. 2), a “sigmoid bubble” (Cover figure), a “filiform bubble” (Fig. 3) and a “hourglass bubble” (Fig. 4).
Beyond the morphology and size of the bubble, the videofluoroscopic examination also enabled the assessment of 2 additional aspects: the presence or absence of residue proximal to the junction (an anatomical parameter) and the degree of tissue elasticity influenced by previous RT (a functional parameter).
Analysis of the videofluoroscopic studies guided the implementation of an integrative speech therapy programme, reserved for patients who had not achieved the expected outcomes during the 10 sessions included in the PORT protocol.
The integrative programme consisted of 10 additional weekly speech therapy sessions, aimed at performing the PORT technique in association with strategies designed to enhance the elasticity of the considered anatomo-physiological district.
Specifically:
- Treatment of irradiated neck tissues using low-frequency vibrations: vibrations generate passive oscillatory movements (“shaking” or “jiggling”) that facilitate water redistribution within the tissues and reduce and/or prevent adhesions;
- Bottom-up elasticity training: regulation and control of sub-valvular phonatory pressure using a dedicated manometer. Lowering the pressure required for phonation promotes greater elasticity in the structures distal to the tracheo-oesophageal prosthesis. Moreover, manometer-based training represents a proprioceptive and awareness-enhancing tool for the patient (Fig. 5).
- Top-down elasticity training: use of semi-occluded vocal tract exercises. This approach produces an inversion of the vocal tract shape (funnel effect), decreasing tract stiffness while simultaneously modifying supra-sphincteric pressure (shifting from negative to positive), thereby reducing rigidity at the pharyngoesophageal junction and promoting vibration (Fig. 6).
- Active mobilisation of head-neck-shoulder muscular structures.
Olfactometric testing, CCS, and UW-QoL v4 assessments were performed at 3 time-points: before the beginning of rehabilitation, after completion of the 10 PORT sessions, and at the 6-month follow-up. However, for patients requiring the integrative programme, these assessments were repeated upon its completion.
Videofluoroscopy – already part of the routine follow-up pathway – was performed at the end of the PORT rehabilitation programme and at the 6-month follow-up.
Statistical analysis
DESCRIPTIVE ANALYSIS
Patients (n = 31) were divided into 2 groups based on their olfactory recovery outcome (PORT performance) at the end of standard therapy (10 sessions):
- Group A (n = 15): patients who recovered olfaction following the standard PORT protocol (favourable outcome);
- Group B (n = 16): patients who did not recover olfaction and were therefore referred to the integrative speech therapy programme.
Anatomical characteristics observed on videofluoroscopic swallowing study (VFSS), particularly the morphology of the PAB, were summarised using contingency tables (pivot tables) to describe frequency distributions across the 2 clinical groups.
INFERENTIAL ANALYSIS
To assess whether the distribution of PAB morphology was significantly associated with the outcome of PORT treatment, Pearson’s Chi-Square test (χ2) was used.
1. Association between PAB morphology and clinical outcome
The χ2 test was applied to the contingency table crossing the variable Bubble Morphology (regular, sigmoid, distal development, filiform, hourglass) with Clinical Group (Group A vs Group B).
The results demonstrated a statistically significant association (p < 0.05) between PAB morphology and olfactory recovery outcome: χ2(4) = 10.15, p = 0.038.
This significant result supports the hypothesis that PAB morphology is not randomly distributed between patients responding positively to standard PORT treatment and those requiring the integrative pathway.
2. Specificity analysis (descriptive post-hoc assessment)
Descriptive frequency analysis showed that regular morphology was clearly predominant in Group A (73.3%), whereas more complex morphologies (distal development, filiform, hourglass) were observed exclusively in Group B (Fig. 7).
Additional χ2 tests were run to correlate individual VFSS parameters (bubble size, elasticity, sub-valvular pressure, and presence of stasis) with the different morphologies to support functional interpretation (Fig. 8).
Results
Videofluoroscopic studies, performed between February and October 2022, were analysed for 31 patients (20 males, 11 females) treated with the PORT rehabilitation protocol. Mean age was 69 years. Thirty patients underwent primary TL, and one underwent salvage TL for local recurrence after partial laryngectomy.
Of the 31 patients, 15 recovered olfaction at the end of the standard 10-session PORT program (Group A), whereas 16 required the integrative speech therapy pathway (Group B) (Figs. 9-12).
Among the 15 patients of Group A with favourable PORT outcomes, 11 showed a regular PAB morphology and 4 a sigmoid morphology.
Among the 16 patients of Group B, 8 had a regular morphology, 3 distal-development, 2 filiform, 2 sigmoid, and one hourglass morphology (Fig. 7).
The analysis revealed correlations among several parameters: PAB morphology, size, elasticity/stiffness, presence/absence of residue proximal to the pharyngoesophageal junction, and sub-valvular pressure measured using a dedicated manometer.
- Group A (regular morphology):
- 11 cases, 9 with medium-sized bubbles, preserved elasticity, no residue, adequate sub-valvular pressure; 2 with larger bubbles but otherwise normal parameters (likely related to surgical configuration);
- sigmoid bubbles showed preserved elasticity, absence of residue, and adequate pressure.
- Group B:
- regular morphology: all 8 cases had large bubble size, residue, reduced elasticity, and inadequate pressure;
- distal-development: all medium-sized with reduced elasticity; one case with residue and adequate pressure; 2 cases without residue but with inadequate pressure;
- filiform: small size, residue, reduced elasticity, inadequate pressure;
- sigmoid: residue, reduced elasticity, inadequate pressure;
- hourglass: medium size, no residue, but inadequate pressure and reduced elasticity.
Discussion
Analysis of the correlations among parameters shows that, for regular-morphology PABs, size is particularly relevant for favourable PORT outcomes. Medium-sized bubbles (Group A) corresponded to adequate functionality across all other parameters. Conversely, large regular bubbles in Group B reflected excessive sub-valvular pressure combined with stasis at the pharyngoesophageal junction, resulting in segmental distension.
The 2 cases of large regular bubbles in Group A – despite preserved functionality – likely reflect structural variations inherent to surgical outcomes.
Sigmoid bubbles did not interfere with PORT acquisition unless accompanied by residue, reduced elasticity, or inadequate pressure. When present, multiple “sniffs” during training helped clear stagnant odorant residues.
Distal-development bubbles were mostly associated with excessive sub-valvular pressure due to distal rigidity; increased resistance to expiratory airflow diverted air distally, producing dilation. One case instead reflected predominant pharyngoesophageal stiffness, demonstrated by upstream residue.
Filiform bubbles represented rigidity both at the pharyngo-oesophageal junction and distal structures.
In the single hourglass case, the intermediate narrowing significantly reduced lumen calibre and thus air passage, compromising olfactory recovery.
Only 3 patients failed to recover olfaction despite integrative therapy: 2 with filiform morphology and one with hourglass morphology.
In filiform cases, post-radiation fibrosis at the junction and distal tract prevented adequate airflow needed for both olfactory recovery and functional tracheo-oesophageal voicing (producing perceptually strained voice).
In one of these patients, mechanical dilation of the proximal oesophagus was required due to concomitant swallowing impairment.
Conclusions
When evaluating this work, it is important to acknowledge the limitation represented by the relatively small sample size, which renders its findings preliminary.
Nevertheless, the results indicate that PORT is an effective rehabilitative technique even in anatomically and physiologically complex cases of laryngectomised patients with tracheo-oesophageal prostheses.
A careful interpretation of the neo-physiology is essential for assessing treatment efficacy, as 28 of the 31 rehabilitated patients achieved a physiological restoration of the daily “olfactory gesture,” albeit with different modalities and timing.
Therefore, PORT emerges as a widely applicable and highly effective technique for the vast majority of laryngectomised patients with tracheo-oesophageal prostheses.
However, the relatively recent introduction of trachea-oesophageal prostheses into routine clinical practice limits long-term understanding of their anatomical, functional, and rehabilitative implications. Videofluoroscopy thus becomes a dynamic window into the post-TL new anatomy and physiology, enabling therapeutic insights grounded in direct observation of the functioning of the rhino-pharyngo-oesophageal tract and representing a highly valuable tool for rehabilitation specialists.
The association between outcomes of olfactory rehabilitation with PORT and the videofluoroscopic assessment of post-TL iatrogenic changes has highlighted a set of anatomo-functional correlations that, in specific cases, required a revision of the rehabilitation protocol – leading to the development of an integrative pathway to achieve the desired result.
Acknowledgements
The authors would like to thank all the patients who participated in the study.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
MG: conceptualization, methodology, investigation, resources, editing - original draft preparation, writing - review and editing; SS, AM: software, formal analysis; DPV, DAL, TG: validation; MG, SS: data curation; TG: visualization; DAL: supervision; DPV: project administration. All authors have read and agreed to the published version of the manuscript.
Ethical consideration
The study was conducted in accordance with the principles of the Declaration of Helsinki. All participants provided informed consent to participate in the study.
History
Received: March 23, 2026
Accepted: April 8, 2026
Figures and tables
Figure 1. Proximal oesophageal phonatory air bubble (PAB) with regular morphology, large size (A) and medium size (B), associated with residue. Proximal oesophageal PAB with regular morphology, large size, without residue (C).
Figure 2. Proximal oesophageal PAB with irregular morphology: “distally developing bubble”.
Figure 3. Proximal esophageal PAB with irregular morphology: “filiform bubble”.
Figure 4. Proximal oesophageal PAB with irregular morphology: “hourglass-shaped bubble”.
Figure 5. Bottom-up elasticity training: management and regulation of sub-valvular phonatory pressure using a dedicated manometer.
Figure 6. Top-down elasticity training.
Figure 7. Distribution (%) of PAB morphologies in Groups A and B.
Figure 8. Correlation between stasis, sub-valvular pressure, and PAB morphology.
Figure 9. Trend of mean olfactometry values across the 3 assessment points (T0, T1, T2). The figure shows a progressive and statistically significant improvement in olfactory performance following the rehabilitative treatment.
Figure 10. Evolution of quality of life (UW-QoL v4) in laryngectomised patients of Group A and Group B treated with the PORT protocol: significant improvement from baseline to post-treatment, with maintenance of the benefit at follow-up.
Figure 11. Trend of the CCS Smell (0-6) for Group A and Group B across T0, T1, and T2.
Figure 12. Trend of the CCS Taste (0-10) for Group A and Group B across T0, T1, and T2.
References
- Ceachir O, Hainarosie R, Zainea V. Total laryngectomy – Past, present, future. Maedica (Bucur). 2014;9:210-216.
- Saad T, Alghalbi S, Aldawsari G. Total laryngectomy, consequences and outcomes: an overview. Int J Healthcare Sci. 2016;4:1853-1860.
- de Luca P, de Campora L, Gallo O. “Almost forty!”: four decades of open partial horizontal laryngectomy – The evolving experience of the Italian School of Enrico de Campora. Head Neck. 2025;47:1364-1371. doi:https://doi.org/10.1002/HED.28041
- Li M, Lorenz R, Khan M. Salvage laryngectomy in patients with recurrent laryngeal cancer in the setting of nonoperative treatment failure. Otolaryngol Head Neck Surg. 2013;149:245-251. doi:https://doi.org/10.1177/0194599813486257
- Hanna E, Sherman A, Cash D. Quality of life for patients following total laryngectomy vs chemoradiation for laryngeal preservation. Arch Otolaryngol Head Neck Surg. 2004;130:875-879. doi:https://doi.org/10.1001/ARCHOTOL.130.7.875
- Fujii M, Fukazawa K, Hatta C. Olfactory acuity after total laryngectomy. Chem Senses. 2002;27:117-121. doi:https://doi.org/10.1093/CHEMSE/27.2.117
- Parbst F, Kostka J, Günther A. Developmental olfactory dysfunction and abnormal odor memory in immune-challenged Disc1+/− mice. J Neurosci. 2025;45. doi:https://doi.org/10.1523/JNEUROSCI.1007-24.2025
- Hilgers F, Ackerstaff A, Aaronson N. Physical and psychosocial consequences of total laryngectomy. Clin Otolaryngol Allied Sci. 1990;15:421-425. doi:https://doi.org/10.1111/J.1365-2273.1990.TB00494.X
- van Dam F, Hilgers F, Emsbroek G. Deterioration of olfaction and gustation as a consequence of total laryngectomy. Laryngoscope. 1999;109:1150-1155. doi:https://doi.org/10.1097/00005537-199907000-00027
- Hilgers F, Van Dam F, Keyzers S. Rehabilitation of olfaction after laryngectomy by means of a nasal airflow-inducing maneuver: the “polite yawning” technique. Arch Otolaryngol Head Neck Surg. 2000;126:726-732. doi:https://doi.org/10.1001/ARCHOTOL.126.6.726
- Moor J, Rafferty A, Sood S. Can laryngectomees smell? Considerations regarding olfactory rehabilitation following total laryngectomy. J Laryngol Otol. 2010;124:361-365. doi:https://doi.org/10.1017/S0022215109992489
- Spadera L, De Luca P, Viola P. A new olfactory rehabilitation protocol based on physiological induction of nasal airflow after total laryngectomy: the Physiological Olfactory Recovery Technique (PORT). Support Care Cancer. 2025;33. doi:https://doi.org/10.1007/S00520-025-09766-2
- Hummel T, Sekinger B, Wolf S. “Sniffin” sticks’: olfactory performance assessed by the combined testing of odor identification, odor discrimination and olfactory threshold. Chem Senses. 1997;22:39-52. doi:https://doi.org/10.1093/CHEMSE/22.1.39
- Risberg-Berlin B, Rydén A, Möller R. Development of a clinical instrument improving rehabilitation of olfaction with the Nasal Airflow-Inducing Maneuver in Swedish laryngectomized patients. Acta Otolaryngol. 2009;129:1026-1032. doi:https://doi.org/10.1080/00016480802495404
- Heald A, Pieper C, Schiffman S. Taste and smell complaints in HIV-infected patients. AIDS. 1998;12:1667-1674. doi:https://doi.org/10.1097/00002030-199813000-00015
- Rogers S, Gwanne S, Lowe D. The addition of mood and anxiety domains to the University of Washington quality of life scale. Head Neck. 2002;24:521-529. doi:https://doi.org/10.1002/HED.10106
- Wald T, Wichmann G, Dietz A. Update on larynx organ preservation in locally advanced laryngeal and hypopharyngeal carcinoma. Laryngorhinootologie. 2025;104:667-680. doi:https://doi.org/10.1055/A-2473-5906
Downloads
License

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Copyright
Copyright (c) 2026 Società Italiana di Otorinolaringoiatria e chirurgia cervico facciale
How to Cite
- Abstract viewed - 329 times
- PDF downloaded - 101 times